


Introduction
Nontuberculous mycobacteria (NTM) are generally classified as either slow or rapid growers. Rapidly growing mycobacteria (RGM), which are characterized by visible growth on solid media within 7 days, include three clinically relevant species, Mycobacterium fortuitum, M. abscessus, and M. chelonae1-3. All are environmental microorganisms found in soil, bioaerosols, and natural and chlorinated water1-3. RGM lung disease is predominantly due to M. abscessus (80% of cases) and M. fortuitum (15% of cases)4,5. M. chelonae usually causes skin, bone, and soft tissue infections and is a very rare respiratory pathogen6,7. Here, we report a case of M. chelonae lung disease associated with bronchiectasis in a previously healthy woman.
Case Report
In April 2008, a 69-year-old woman was referred to our hospital because of hemoptysis. She had been healthy until one month prior, when intermittent hemoptysis developed. The patient had no smoking history or other medical history. On examination, the patient appeared well. Her weight was 45 kg, height 156.2 cm, temperature 36.2℃, blood pressure 133/75 mm Hg, pulse 73 beats per minute, and oxygen saturation 100% while breathing ambient air. Laboratory results were normal. A human immunodeficiency virus antibody test was negative.
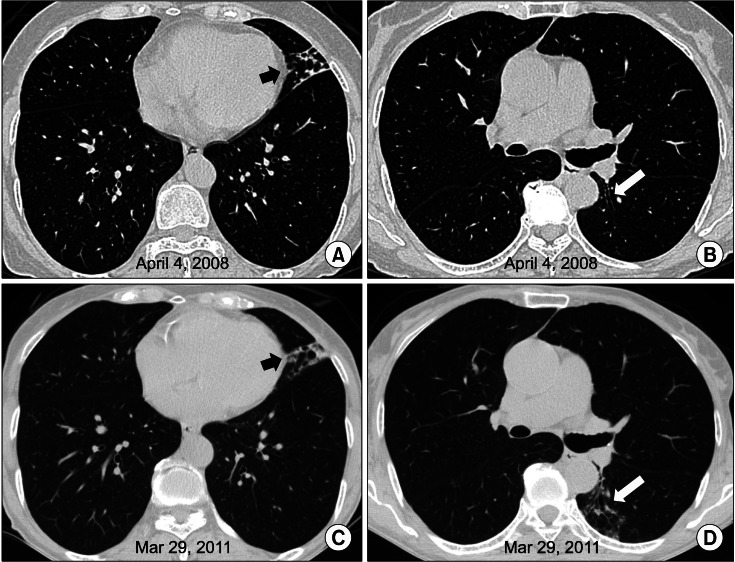
A computed tomography (CT) scan of the chest revealed bronchiectasis and bronchiolitis in the lingular division of the left upper lobe (Figure 1A, B). There was no evidence of cystic fibrosis or other common causes of bronchiectasis. NTM were isolated three times from sputum specimens.
NTM species were identified using a polymerase chain reaction-restriction fragment length polymorphism analysis (PRA) based on the partial region of the rpoB gene8. Colonies were scraped, and genomic DNA of the isolate was extracted using a commercial kit (QIAamp DNA Mini kit; Qiagen, Hilden, Germany). Amplification of the partial rpoB gene (360 bp) was performed using primers Rpo5' (5'-TCAAGGAGAAGCGCTACGA-3') and Rpo3' (5'-GGATGTTGATCAGGGTCTGC-3')8 with subsequent digestion with 5 units of Msp I (New England BioLabs, Beverly, MA, USA) for 3 hours at 37℃. The digestion mixtures were analyzed by 3% (w/v) agarose gel electrophoresis. DNA size markers, pBR322-MspI-digested DNA (New England BioLabs) were used to enable estimation of DNA fragment size. The PRA results were determined by comparing their restriction patterns with those available in the National Center for Biotechnology Information GenBank database9 and referred to as described by Lee et al.8 for the rpoB-PRA. The rpoB amplicon restricted by MspI resulted in fragment sizes of 105, 95, 80, 50, and 40 bp in two serial cultures (Figure 2). The rpoB-PRA patterns of those cultures exactly matched the known restriction fragment pattern of the reference strain of M. chelonae subsp. chelonae ATCC35749.
The identification of these NTM isolates was further confirmed by DNA sequence analysis of the partial rpoB gene (723 bp) using primers MycoF (5'-GGCAAGGTCACCCCGAAGGG-3') and MycoR (5'-AGCGGCTGCTGGGTGATCATC-3')10 and the partial hsp65 gene (439 bp) using primers Tb11 (5'-ACCAACGATGGTGTGTCCAT-3') and Tb12 (5'-CTTGTCGAACCGCATACCCT-3'). The results revealed sequence similarity (above 99.9%) with M. chelonae for the rpoB gene (GenBank accession no. EU109300.1) and hsp65 gene (GenBank accession no. U55832).
Finally, the patient was diagnosed with M. chelonae lung disease. Antibiotic therapy was not initiated because of her mild symptoms. Three years after diagnosis of M. chelonae lung disease, follow-up chest CT was performed. Although there was mild progression of peribronchial infiltration on the lingular division of the left upper lobe and newly appeared bronchiolitis in the superior segment of the left lower lobe (Figure 1C, D), she did not complain of aggravation of her symptoms.
Discussion
The nomenclature of RGM has changed frequently and has been a source of confusion for clinicians. For instance, within the past approximately 20 years, M. abscessus, the most common RGM respiratory pathogen, was labeled as M. cheloneii subsp. abscessus, M. chelonae subsp. abscessus, and finally, in 1992, M. abscessus11. Unfortunately, some mycobacterial laboratories still report M. abscessus isolates as M. chelonae complex or M. chelonae/abscessus group without further species identification12,13. The species identification is important because therapy differs significantly depending on the RGM species obtained. Because M. chelonae is an extremely rare cause of pulmonary disease, most respiratory isolates that are identified as M. chelonae/abscessus complex can be reasonably assumed to be M. abscessus isolates2.
Identifying RGM to the species level is very important1-3. Biochemical tests that assess phenotype characteristics have commonly been used by clinical laboratories to characterize RGM. However, these are time-consuming and do not always lead to identification of the organism to the species level2,3. High-performance liquid chromatography, which is a useful method for identifying slowly growing NTM, may not enable separation of M. chelonae and M. abscessus2,3. Molecular methods can provide reliable and rapid identification of RGM1. In this study, the M. chelonae isolates were identified using rpoB gene based-PRA and sequence analysis of the rpoB and hsp65 genes.
Skin, bone, and soft tissue disease are the most important clinical manifestations of M. chelonae infection. Disseminated M. chelonae infection can also occur in immunocompromised patients1. M. chelonae is an increasingly recognized cause of keratitis, especially after injury with a foreign body or following office ophthalmologic procedures1. However, M. chelonae is a much less frequent cause of lung disease than M. abscessus1-3.
Reported cases of M. chelonae lung disease are usually middle-aged or elderly women with no other co-existing parenchymal lung disease. The symptoms and radiographic presentation of M. chelonae lung disease are similar to those of other RGM lung diseases5. Bronchiectasis, nodules, and consolidation are the most common CT features14.
It is important to distinguish M. chelonae from M. abscessus because therapy for M. chelonae is potentially easier than for M. abscessus infection1. M. chelonae is resistant to anti-tuberculosis agents but is susceptible to a number of traditional anti-bacterial agents such as tobramycin (100%), clarithromycin (100%), linezolid (90%), imipenem (60%), amikacin (50%), clofazimine, doxycycline (25%), and ciprofloxacin (20%)1. In addition, inducible resistance to clarithromycin which is conferred by an erm (41) gene is found in M. abscessus but is absent from M. chelonae15.
In conclusion, M. chelonae should be considered a possible etiologic pathogen of the nodular bronchiectatic form of NTM lung disease, despite the rarity of pulmonary M. chelonae infection. To the best of our knowledge, this is the first documented case of M. chelonae lung disease in an immunocompetent adult in Korea in which the etiologic organism was confirmed using molecular methods that characterized rpoB and hsp65 gene sequences.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






