


Introduction
Lung cancer is a major cause of death among cancer patients1. In Brazil, it is the cancer with the second highest incidence in men after skin neoplasias, excluding non-melanoma skin cancer2. Some benign diseases can have an unusual presentation, mimicking lung neoplasia in its clinical and radiological manifestations3,4. Thus, separately diagnosing malignant and benign conditions is a frequent challenge in clinical practice5,6.
There should be a balance in the approach to identifying lung lesions and resecting malignant lesions at their initial presentation, and avoiding resecting benign lesion7. Differential diagnosis is essential for the adoption of adequate practices6; in particular, the distinction between benign and malignant lesions is important because the treatment and prognosis of these two disease groups are distinct8. However, lung cancer high incidence and lethality can influence medical decisions and sometimes erroneously direct the diagnostic process to the search for malignant lesions5,9, without including routine tests to diagnose other diseases. Thus, the diagnosis of a potential benign disease is delayed, which negatively affects its progression, increases hospital costs, and exposes patients to unnecessary risks7.
There are few Brazilian studies on the prevalence of diseases that mimic lung cancer. These publications mostly consist of case reports and there is no national studies addressing this topic. Moreover, data from the international literature cannot be extrapolated to our reality because many of these diseases have a variable geographical distribution7, especially infectious diseases endemic to Brazil. Knowledge regarding the prevalence of these diseases within the national epidemiological context is useful for the study of suspected cases of primary lung neoplasm.
Materials and Methods
This study was approved by the Research Ethics Committee of the Federal University of Santa Maria, under number 33554. This is a descriptive cross-sectional study. The data were obtained from medical records of patients hospitalized in the Department of Pneumology at the University Hospital of Santa Maria (HUSM) between September 2003 and September 2013. The HUSM is a tertiary hospital with approximately 300 beds that covers more than 1 million inhabitants in the Central-West region of the state of Rio Grande do Sul, Brazil.
The patients included in this study were Ōēź30 years old and were hospitalized at the HUSM with suspected primary lung cancer, which was suspected if there was a new lung nodular opacity or mass with one of the following findings: hemoptysis, digital clubbing, or weight loss. They underwent invasive diagnostic procedures, including the collection of material for anatomopathological and/or cytopathologic analysis.
These patients were selected from the electronic database of the Information System for Education (SIE) and the search was restricted to the cytopathologic results of specimens collected by fibrobronchoscopy, digital radiography and ultrasound-guided transcutaneous puncture as well as anatomopathological results of lung biopsies obtained via open surgery, fibrobronchoscopy, ultrasound-guided transcutaneous biopsy, and computerized tomography.
A subpopulation of patients for whom cancer diagnosis was excluded via invasive tests was formed and the diagnosis of benign disease was confirmed through pathology or other complementary tests. Carcinoid tumors were considered as malignant lesions when classified as atypical carcinoid tumors due to their aggressive behavior, high metastatic potential, and low mean disease-related survival. Typical carcinoid tumors were considered as benign lesions because they present a good prognosis after surgical treatment, with a reported survival of up to 100% 5 years after resection10.
Patients who were less than 30 years old, those with previous malignant neoplastic disease and without filling lung cancer suspected criteria were excluded from the study.
The medical records of the patients included in the study were reviewed and epidemiological data, diagnosis, radiological characteristics of the lesion, and its location as well as the diagnostic method used were recorded. Subsequently, the collected information were tabulated and analyzed through descriptive statistics using the Statistica StatSoft, Inc. (2009) version 9.1 and the BioEstat 5.0 software (Instituto Bioestat├Łstico de Ci├¬ncia e Tecnologial, 2007).
Results
We identified 1,056 patients who underwent invasive diagnostic procedures and had anatomopathological and cytopathologic test results available in the SIE between September 2003 and September 2013. Of these patients, 252 patients who met the exclusion criteria were excluded and the medical records of 804 patients with suspected primary lung cancer were analyzed.
Definitive diagnosis was obtained in 676 cases (84.1%) and 128 patients (16%) had an inconclusive diagnosis. The group of patients without diagnosis included those who were still undergoing investigative tests, who refused to continue the investigation, or who died without a diagnosis for the suspected lesion. Among patients with established diagnosis, lung neoplasm was confirmed in 622 patients (92.1%) and benign disease was confirmed in 54 patients (8%).
The mean age of the patients with a benign disease diagnosis was 57 years (range, 36-79 years), there was a predominance of males (78%) over females (22%) and 83% of patients had a history of smoking. In most cases, benign diseases had radiological presentation of pulmonary nodule (31.5%), followed by single mass (24.1%), and were found in the lung right superior lobe (20,4%), left superior lobe (11.1%), and right inferior lobe (11.1%).
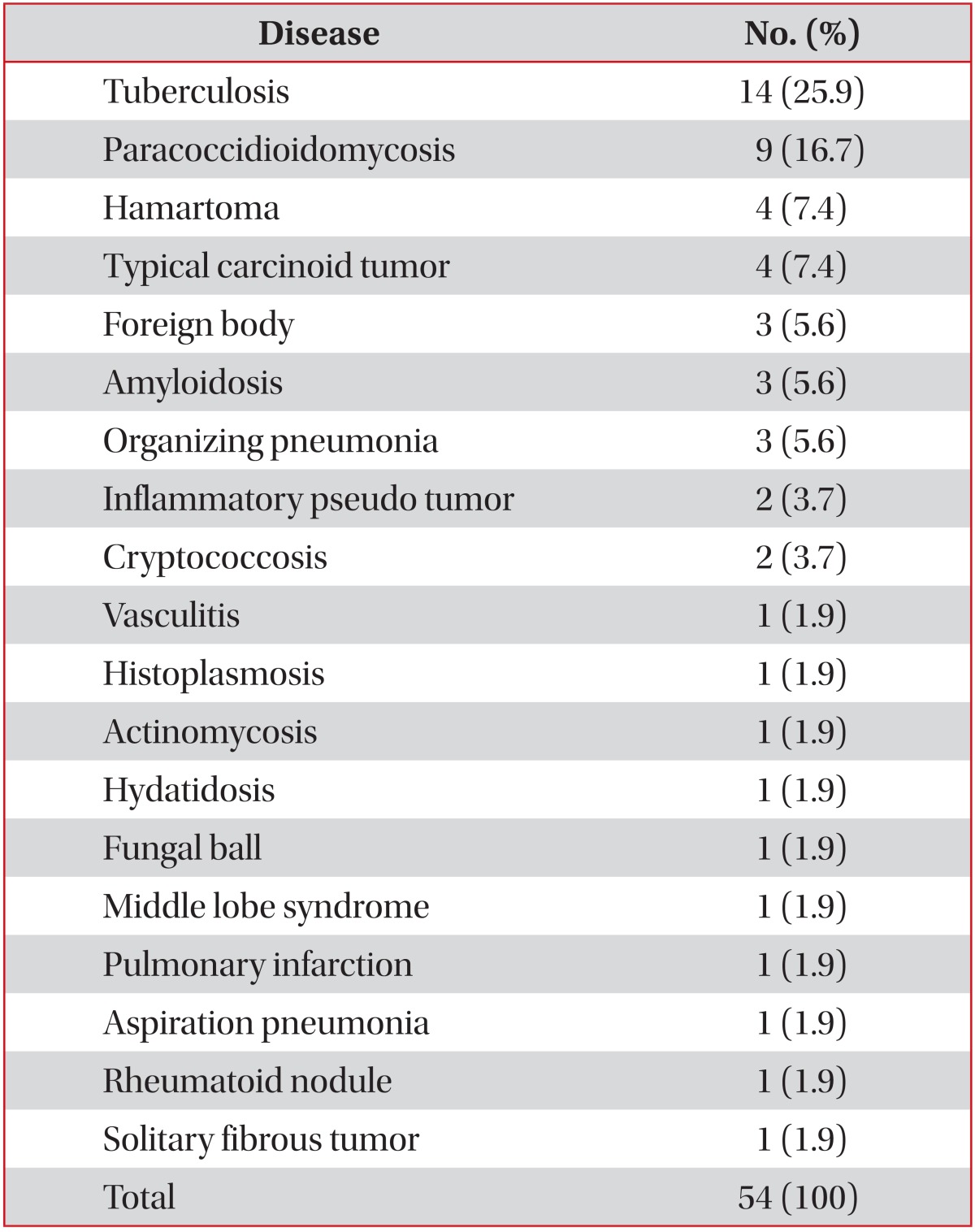
The most frequent diseases were tuberculosis in 14 cases (25.9%), paracoccidioidomycosis in nine cases (16.7%), hamartoma in four cases, and typical carcinoid tumor in four cases (7.4%) (Table 1).
The most frequent subgroup of benign lesions was infectious diseases (55.6%) followed by benign neoplastic diseases (16.7%) and inflammatory diseases (14.9%).
The most frequent infectious disease was tuberculosis in 14 patients, accounting for 46.7% of infectious causes, followed by paracoccidioidomycosis in nine patients (30%) and cryptococosis in two patients (3.4%). Fungal diseases, examined together, accounted for 43.4% of the infections and were only less prevalent than tuberculosis.
The diseases that mimicked cancer were mostly diagnosed via fibrobronchoscopy (55.6%), of which 15 cases were diagnosed by bronchoalveolar lavage and 15 by endobronchial biopsy, followed by surgical procedures (33.3%). Computerized tomography-guided biopsies accounted for only 5.6% of these diagnoses (Table 2, Figures 1, 2, 3).
Discussion
Lung cancer is a frequent condition observed in pneumologist and thoracic surgeon clinical practices. Its prevalence and lethality are a matter of intense concern. Several diseases mimic this condition. These are mostly of infectious etiology and vary according to the epidemiological characteristics of a given region11,12.
In a study conducted in North America, Smith et al.7 found that 9% of benign diseases mimic primary lung cancer. Rolston et al.8 observed a 6.7% prevalence of benign diseases mimicking primary lung cancer. These findings are very similar to ours, which showed an 8% prevalence. However, we observed an important difference in the etiology of these benign lesions when compared to the North American data. Tuberculosis was the most frequent cause of benign diseases observed in our study, which suggests that geographical factors, in particular those associated with infectious diseases, have an essential role in this context.
Factors associated with national epidemiology such as high incidence of granulomatous infectious diseases that present with findings indicative of neoplasm such as tuberculosis, paracoccidioidomycosis, histoplasmosis, actinomycosis, and cryptococcosis tend to increase even further the importance of differential diagnosis in cases of suspected lung cancer.
The tuberculosis incidence rate in Brazil was 35.8/100.000 habitants in 201213, already the incidence of paracoccidioidomycosis is not well established, being estimated at 1-3/100.000 habitants14. These two diseases were the most common infectious etiologies observed in our study, which is in contrast with the study by Smith et al.7 where no cases of these diseases were described. Rolston et al.8 reported that tuberculosis accounted for only 27% of infectious causes and was surpassed by fungal diseases. However, no case of paracoccidioidomycosis was observed.
Taken together, non-infectious benign conditions form an important subgroup, accounting for 44.5% of benign causes. However, it is difficult to compare the prevalence of each disease with that reported in the literature because of the lack of detailed data7,8.
With regard to diagnostic methods, we highlighted the importance of fibrobronchoscopy in the assessment of suspected lung cancer lesions. This minimally invasive method was used for the diagnosis of more than half of the patients studied (55.6%), and there was no record of procedure-related complications. The need for surgical samples was relatively high in our study (33.4%). However, studies published prior to the use of computerized tomography, have described up to 64% of samples from surgical material3,15. In addition, a significant reduction in the use of invasive procedures to establish a diagnosis of lung lesions has been observed in recent decades. Currently, the need for surgery is approximately 9%7. This reduction is probably a result of the improvement and dissemination of less invasive methods with excellent diagnostic yield such as computerized tomography or ultrasound-guided core lung biopsy16.
In all cases of suspected cancer, it is important to obtain the patient's epidemiological and occupational information to estimate the risk of cancer and to perform an accurate analysis of the clinical and radiological presentation of the disease7,17. This information includes factors related to malignancy such as smoking history (in packets/yr), familial and personal history of cancer, advanced age, consumptive symptoms, and hemoptysis17,18,19. Moreover, it should be investigated whether the patient was in endemic regions for systemic mycoses, especially for men living in rural areas20. Similarly, history of exposure to endemic regions for tuberculosis and, particularly, of contact with patients known to have the bacillus can suggest tuberculosis infection. Alcoholism, poor oral hygiene, and history of orofacial trauma are indicative of actinomycosis11.
In this study, the patients with benign lung disease exhibited a high prevalence of smokers (83%). The fact that the majority of patients were men (78%) and farmers (73%), and that the South region of Brazil is an endemic area for paracoccidioidomycosis14,20 explains the high incidence of this disease, as opposed to the series of cases previously reported in the literature7,8.
The high number of inconclusive results in pathological analyses could be considered as one limitation of this study. Many of these could indicate benign diseases mimicking cancer due to the absence of malignant cells in the analyzed samples, which would increase the prevalence of these diseases in the study. However, these results were not included owing to the absence of an accurate diagnosis. Despite this limitation, the persistent search for differential diagnoses through a diagnostic routine provided a significant number of alternative diagnoses, and the rate of benign conditions was similar to North American studies. This demonstrated that the search for differential diagnoses should not be limited by the lack of complementary tests and that other methods that may be more invasive, but that detect the cause of the disease, should be used to offer an appropriate treatment to the patients.
In conclusion, this study reinforces that the diagnosis of diseases that mimic lung cancer depends on their geographical distribution and that infectious diseases, in particular tuberculosis and paracoccidioidomycosis, should always be taken into consideration in the differential diagnosis of patients with suspected pulmonary neoplasm. In addition, a diagnostic routine for these diseases, with the adequate collection and storage of clinical specimens and laboratory evaluation using adequate staining and culture media, can lead to a diagnosis without the need for high-cost procedures.




 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






