



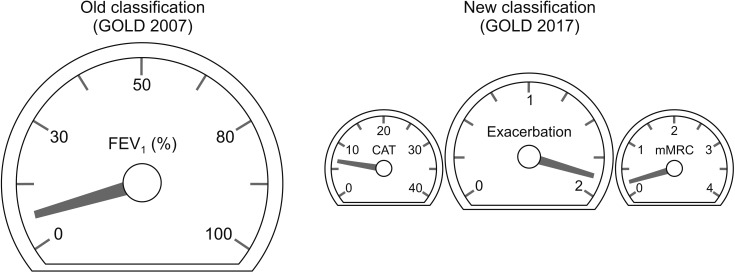
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable disease which is characterized by respiratory symptoms and airflow limitation1. It is a leading cause of death in worldwide. Classification of COPD is very important since treatment is recommended by classification. Old COPD classification is based on spirometry result. In Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2007 document2, post bronchodilator forced expiratory volume in 1 second (FEV1) measured by spirometry was used to classify COPD. FEV1 is easy to measure and result is quite consistent. Moreover, measurement of FEV1 is standardized worldwide. There is no room for bias in measuring FEV1. GOLD 2007 classified COPD as stage I to IV based on post bronchodilator FEV1(%).
In 2011, GOLD committee changed classification of COPD from I-IV to ABCD. Main reason for this change is that there was some discrepancy between lung function and quality of life3. Moreover, history of exacerbation is more powerful predictor for future exacerbation than FEV1 (%)4. Later in 2017, FEV1 (%) was removed from criteria for classification between high and low risk groups1. Spirometry result is still mandatory when diagnose of COPD. However, it is no longer considered when classifying COPD patients (Figure 1).
Since the release 2017 GOLD documents, there have been debates whether GOLD 2017 classification is better than old spirometric classification. Gedebjerg et al.5 showed that GOLD 2017 classification does not predict mortality more accurately than 2007. Data from PLATINO study showed that GOLD 2007 classification shows more stability over time compared with GOLD 2013.6 Recently, Candemir et al.7 investigated whether there was a difference between GOLD 2017 classification and 2007 in clinical variables in patients with COPD. Interestingly, similar values of FEV1 were found between group A and C. Also, mean FEV1 was not different at all between B and D. Moreover, group A and C showed similar result of incremental shuttle walk test (ISWT). On the contrary, GOLD 2007 classification was well correlated with many clinically important variables such as dyspnea, quality of life, anxiety scores, body mass index, fat free mass index, and ISWT.
These previous results showed that still FEV1 (%) is good and useful markers for classification of COPD. It is not yet concluded whether removal of FEV1 in GOLD 2017 was good decision or not. However, as the Candemir et al.7 mentioned, GOLD 2017 classification might not represent the severity of COPD sufficiently well. Probably the combination of both spirometric stage and combined assessment of GOLD 2017 is important, especially for estimating clinical variables.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






