Duration of Pulmonary Tuberculosis Infectiousness under Adequate Therapy, as Assessed Using Induced Sputum Samples
Article information
Abstract
Background
A sputum culture is the most reliable indicator of the infectiousness of pulmonary tuberculosis (PTB); however, a spontaneous sputum specimen may not be suitable. The aim of this study was to evaluate the infectious period in patients with non–drug-resistant (DR) PTB receiving adequate standard chemotherapy, using induced sputum (IS) specimens.
Methods
We evaluated the duration of infectiousness of PTB using a retrospective cohort design.
Results
Among the 35 patients with PTB, 22 were smear-positive. The rates of IS culture positivity from baseline to the sixth week of anti-tuberculosis medication in the smear-positive PTB group were 100%, 100%, 91%, 73%, 36%, and 18%, respectively. For smear-positive PTB cases, the median time of conversion to culture negativity was 35.0 days (range, 28.0–42.0 days). In the smear-negative PTB group (n=13), the weekly rates of positive IS culture were 100%, 77%, 39%, 8%, 0%, and 0%, respectively, and the median time to conversion to culture-negative was 21.0 days (range, 17.5–28.0 days).
Conclusion
The infectiousness of PTB, under adequate therapy, may persist longer than previously reported, even in patients with non-DR PTB.
Introduction
Tuberculosis (TB) has been the leading cause of death worldwide; an estimated one billion people have died from TB in the past 200 years1. Despite the global effort to control TB, it remains a massive threat to global health. In 2012, 8.6 million new TB cases, 1.3 million human immunodeficiency virus (HIV)–negative TB deaths, and 0.35 million HIV-positive TB deaths were reported2. To prevent and interrupt pulmonary tuberculosis (PTB) transmission, emphasis should be placed on the early detection, early initiation of appropriate treatment, and adequate infection control measures.
Almost all PTB cases are transmitted through the airborne route3. Several factors are known to contribute to the infectiousness of a PTB patient4. Studies have reported that most PTB patients are no longer infectious after 2 weeks of treatment due to a reduction in coughing and a decrease in viable Mycobacterium tuberculosis (MTB), such that their infectiousness is 50-times less than before anti-TB medication initiation567891011. In fact, several TB guidelines define the determining factor for becoming noninfectious, even for patients with smear-positive PTB without any risk factor for multi-drug resistant (DR) TB, as the administration of standard multidrug anti-TB therapy for 2–3 weeks34121314.
However, the relative infectiousness is associated with positive sputum culture results and is highest when the smear results are also positive13. Moreover, it is well known that 13%–41% of new TB cases are transmitted from smear-negative but culture-positive patients151617. Therefore, sputum culture status is the most reliable and useful indicator of a patient's infectiousness14. Fitzwater et al.18 reported that the median conversion time from culture-positivity to culture-negativity under anti-TB medication is 37 days, which is longer than previously reported.
An induced sputum (IS) specimen is more useful for pathogen detection in suspected PTB cases than a spontaneous sputum specimen. This is especially true when a patient's spontaneous sputum specimen is smear microscopy negative, the patient is unable to expectorate spontaneously, or when the produced sputum is inadequate in amount or quality192021. Anderson et al.22 reported that the diagnostic accuracy of an IS specimen is equivalent to that of bronchoscopy for the diagnosis of smear-negative PTB.
The reduction in coughing after anti-TB therapy limits the effectiveness of spontaneous sputum specimen in evaluating the infectiousness of PTB. However, no study has evaluated the change in infectiousness of treated PTB patients using repeated IS samples. Therefore, the aim of this study was to evaluate the infectious period in PTB patients fully susceptible to isoniazid (INH), rifampicin (RIF), ethambutol (EMB), and pyrazinamide (PZA) using weekly serial IS specimens while receiving adequate standard anti-TB chemotherapy.
Materials and Methods
1. Study population and design
This was a retrospective study performed in a cohort of patients diagnosed with PTB between March 2013 and February 2015 at the Inje University Busan Paik Hospital (a 903-bed, university-affiliated, tertiary referral hospital in Busan, Republic of Korea). Since March 2013, IS has been performed for patients with presumptive and microbiologically confirmed PTB at our hospital in a single outpatient room, ventilated directly to the outside. The protocol for this study was approved by the Institutional Review Board of Busan Paik Hospital (IRB No. 15-0194) and allowed review and publication of information from patient records. Informed consent was waived owing to the retrospective nature of the study, and patient information was anonymized prior to analysis.
Consecutive patients aged >20 years with a PTB diagnosis, and undergoing an IS, were screened for this study. To evaluate the smear and culture conversion rates after the commencement of anti-TB medication in non-DR PTB patients, the enrollment criteria were (1) patients diagnosed with microbiologically confirmed PTB and (2) patients who underwent IS before the PTB diagnosis and weekly thereafter for the first 6 weeks after the commencement of anti-TB medication. The exclusion criteria were (1) patients who had received any anti-TB treatment before the baseline IS; (2) patients who received prior PTB treatment, defined as ≥1-month history of TB treatment; (3) patients with DR-PTB including resistance to INH, RIF, EMB, or PZA; (4) patients who had discontinued the standard anti-TB medication (containing INH, RIF, EMB, and PZA) due to adverse drug reactions including hepatitis and skin rash during the first 6 weeks.
2. IS procedure
The IS procedure was performed by trained nurses in a procedure room in the outpatient unit. Each IS comprised three procedural steps: (1) administration of 2 mL of salbutamol via a mouthpiece using an ultrasonic nebulizer (Pari Boy SX, Pari GmbH, Starnberg, Germany), (2) administration of 20 mL of 3% hypertonic saline using a nebulizer over a period of 20 minutes, and (3) sample collection following spontaneous expectoration of 1–20 mL sputum over the next 10–30 minutes14232425. IS was not performed in patients with a history of airway hyperresponsiveness or bronchoconstriction including asthma and chronic obstructive pulmonary disease, or an oxygen saturation level below 90% in ambient air, because of the possibility of deterioration of their condition2324.
3. Microbiologic examination of IS
All IS specimens were processed and pretreated in accordance with the recommended standard techniques for mycobacterial examination of sputum samples26. Acid-fast bacilli (AFB) smears of IS were examined following auramine–rhodamine fluorescence staining and graded on a scale of 0 to 4+27. All IS specimens were simultaneously cultured on both solid media (SM) and liquid media (LM) using 3% Ogawa medium (Eiken Chemical, Tokyo, Japan) and the mycobacterial growth indicator tube 960 system (Becton Dickinson, Mountain View, CA, USA). All MTB isolates from the baseline IS specimens were sent for drug sensitivity testing to the Korean Institute of Tuberculosis (KIT), a World Health Organization-designated supranational reference laboratory. At KIT, resistance to anti-TB agents was defined as mycobacterial growth above 1% in Löwenstein-Jensen medium, using the proportional method.
4. Classification of parenchymal lesions in PTB
We identified the presence or absence of cavitation of PTB based on chest computed tomography (CT). The extent of the parenchymal lesion was categorized on the basis of the lobar involvement seen in the chest CT.
5. Data analysis
The results presented in the text and tables are expressed as median values and interquartile ranges or as numbers (%). The data were compared using the Mann-Whitney U test for continuous variables, and using the Pearson's chi-square test or Fisher exact test for categorical variables. Cumulative percentage curves of positive-to-negative culture conversion according to PTB patients' AFB smear status were generated using the Kaplan-Meier method and the curves were compared using the log-rank test. All comparisons were two-sided, and a p-value <0.05 was considered to indicate statistical significance. Data were analyzed using IBM SPSS Statistics version 19 (IBM Corp., Armonk, NY, USA).
Results
1. Patient characteristics
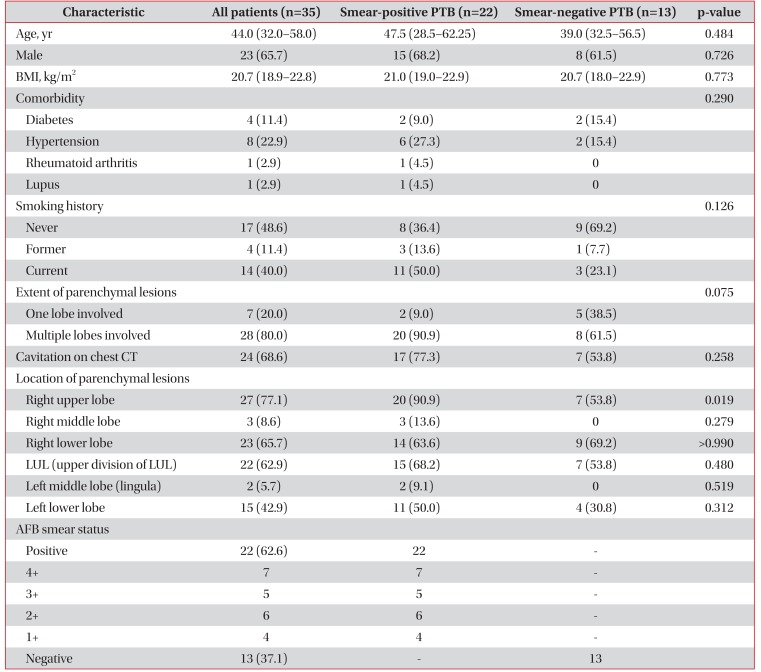
During the study period, 773 patients were diagnosed with PTB. Of these, 41 patients underwent IS before the PTB diagnosis and a weekly IS thereafter for the first 6 weeks of receiving anti-TB medication. Six patients were excluded because they had DR-PTB (two resistant to INH only, one resistant to INH and EMB, and one resistant to RIF and EMB or because they had discontinued anti-TB medication because of hepatitis [n=1] or skin rash [n=1]). Finally, 35 PTB patients were included in the study and analyzed. The demographic and descriptive data of the enrolled patients are summarized in Table 1. Of the 35 enrolled PTB patients, 22 (63%) were AFB smear-positive and the remaining 13 (37%) were AFB smear-negative. The enrolled patients were predominantly male and were classified as having PTB with multilobar involvement. None of the enrolled patients were co-infected with HIV.

Demographic and clinical characteristics of enrolled 35 patients diagnosed with PTB who underwent induced sputum culture for 6 consecutive weeks
2. Overall trend of positive-to-negative culture conversion assessed by weekly IS after commencement of appropriate standard anti-TB medication
The overall trend of positive-to-negative culture conversion in the 35 enrolled patients is shown in Figure 1A. After 2 weeks of anti-TB medication, 86% and 37% of the patients remained culture-positive for MTB in LM and SM, respectively. After 4 and 6 weeks, 49% and 6% of the cultures in LM and 9% and 0% of the cultures in SM were positive for MTB. The median conversion time from culture positivity to culture negativity for all patients was 28.0 days (range, 21.0–35.0 days).
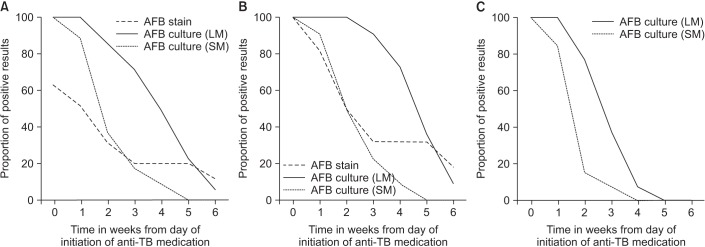
Trends of positive-to-negative culture conversion assessed by weekly serial induced sputum after adequate standard anti-tuberculosis medication. Positive-to-negative culture conversion trend based on acid-fast bacilli (AFB) smear status, as assessed using weekly induced sputum specimens. (A) Overall trend of positive-to-negative culture conversion (n=35). (B) Trend of positive-to-negative culture conversion in smear-positive pulmonary tuberculosis (n=22). (C) Trend of positive-to-negative culture conversion in smear-negative pulmonary tuberculosis (n=13). LM: liquid media; SM: solid media.
3. Positive-to-negative culture conversion trend based on AFB smear status, as assessed using weekly IS specimens
Figure 1B and C show the different rates of conversion of PTB to culture negative according to AFB smear status, smear positive or smear negative. The results for the 22 smear-positive PTB patients in Figure 1B show that all patients remained culture positive in LM and 50% remained positive in SM after 2 weeks of appropriate anti-TB medication. Weekly serial IS specimens revealed that despite 4 and 6 weeks of appropriate therapy, 16 (73%) and two (9%) patients remained culture-positive for MTB in LM, respectively while two (9%) and 0 (0%) remained culture-positive in SM, respectively. The median conversion time for the enrolled smear-positive PTB patients to become culture-negative was 35.0 days (range, 28.0–42.0 days). We further assessed the changes in smear microscopy status based on the duration of administered therapy, and as depicted in Figure 1B the smear positivity rates over time were 82%, 50%, 32%, 32%, 32%, and 18%, respectively.
Of the 13 smear-negative PTB patients, 10 (77%) remained culture-positive for MTB in LM, and two (15%) remained positive in SM after 2 weeks of anti-TB medication, as shown in Figure 1C. After 4 weeks of anti-TB medications, one patient (8%) was culture-positive for MTB in LM and none of the 13 patients tested culture-positive in SM. Six weeks after anti-TB therapy initiation, none of the smear-negative PTB patients remained culture-positive in either LM or SM. The median time to conversion for smear-negative PTB patients was 21.0 days (range, 17.5–28.0 days).
We further generated curves for the cumulative percentages of positive-to-negative culture conversions in PTB patients after appropriate standard anti-TB medication according to their AFB smear status but regardless of whether the samples were cultured in SM or LM. As depicted in Figure 2, the percentages of culture conversion were significantly different between patients with smear-positive and smear-negative PTB (p<0.001).
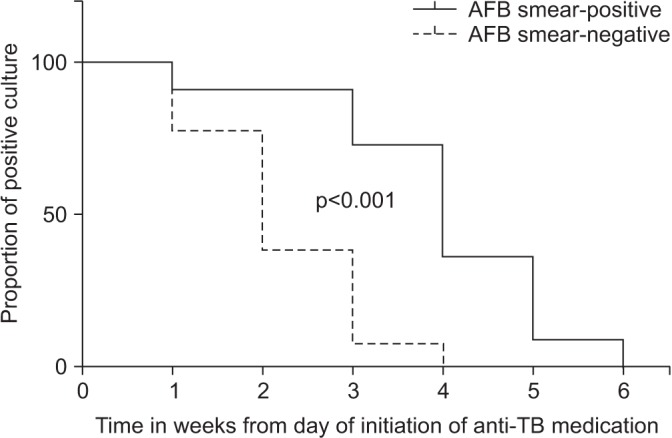
Kaplan-Meier estimates for overall culture positivity according to acid-fast bacilli (AFB) smear status for 35 pulmonary tuberculosis (TB) patients.
4. Overall rate of positive-to-negative culture conversion rates, independent of basal IS, following 4 weeks of anti-TB medication
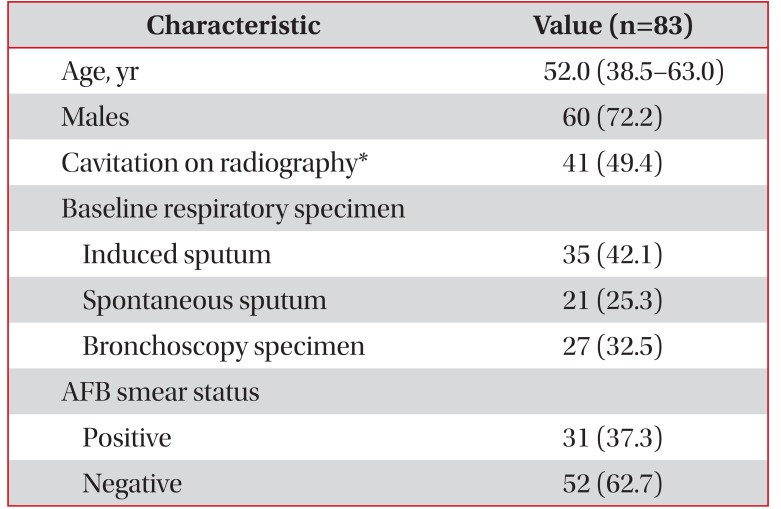
We next estimated the overall positive-to-negative culture conversion rates in our PTB cohort after 4 weeks of therapy by assessing the IS specimens. We performed this analysis for all patients who had an IS specimen available for the fourth week of medication, regardless of whether a basal IS was performed in them. Eighty-three PTB cases were analyzed including the 35 PTB cases that formed our study cohort. The 48 additional cases were selected based on the study's inclusion and exclusion criteria with two points of difference: first, these patients did not undergo IS at the time of PTB diagnosis, and second, they did not undergo weekly IS. PTB was microbiologically confirmed for all 48 cases using bronchoscopy (n=27) or spontaneous sputum (n=21) specimens at the time of diagnosis. The characteristics of the all 83 patients are described in Table 2. Figure 3 shows the proportion of patients who converted to culture-negative after 4 weeks of anti-TB medication. As shown in Figure 3B, 81% of the 31 smear-positive PTB patients remained culture-positive in LM, and 10% remained culture-positive in SM. Further, of the 52 patients with smear-negative PTB, 2% remained culture-positive in LM, and none were culture-positive in SM, as shown in Figure 3C.

Clinical characteristics of 83 patients diagnosed with pulmonary TB who underwent induced sputum culture after 4 weeks of anti-TB medication, regardless of the basal induced sputum results

The rate of positive-to-negative smear and culture conversion assessed by induced sputum after 4 weeks of adequate standard anti-tubuerculosis medication. (A) Overall of positive-to-negative culture conversion (n=83). (B) Positive-to-negative culture conversion in smear-positive pulmonary tuberculosis (n=31). (C) Positive-to-negative culture conversion in smear-negative pulmonary tuberculosis (n=52). AFB: acid-fast bacilli; LM: liquid media; SM: solid media.
Discussion
To the best of our knowledge, this is the first study to evaluate the infectious period of non-DR PTB patients after appropriate standard anti-TB medication, based on the conversion of weekly serial IS specimens to MTB culture-negative. In this study of 35 patients undergoing therapy for PTB, we found that most of these non-DR PTB patients remained culture positive after 2 weeks, although they had previously been considered non-infectious after 2 weeks of treatment. Moreover, more prolonged culture positivity was observed, even in smear-negative PTB patients, than would normally be expected. In particular, more than half of the smear-positive PTB patients remained culture-positive even after 4 weeks of treatment.
It has been postulated that to prevent PTB transmission, and by extension, to reduce the incidence of PTB, an adequate period of isolation is needed for PTB patients. Previous studies reported that an average 2 weeks of treatment with the standard combination of anti-TB medication resulted in a rapid decline in infectiousness, following which, patients were no longer considered infectious78101128. Based on these studies, many published guidelines recommend that 2 weeks of anti-TB therapy is sufficient to reduce infectiousness to a level where isolation is no longer required, although confirmation is not possible until smears are also negative for AFB31314.
However, some recent studies have suggested that this belief may be incorrect. One study showed that 36.7% of HIV-negative and 27.2% HIV-positive smear-positive PTB patients were still AFB positive by sputum microscopy after 2 weeks of adequate therapy29. Dominguez-Castellano et al.30 reported that the median time to conversion to an AFB-negative smear was 28.6 days and that this time was principally dependent on the presence of cavitation, although 12.8% patients in that study had DR-PTB. Parikh et al.31 reported that the median time to conversion of 71 smear-positive PTB patients to negative smear and culture was 5 weeks and 6.5 weeks, respectively. However, because they did not determine the presence of DR-PTB and cultured only on SM, these results may have limited applicability.
Rueda et al.32 reported that in a group of 72 prisoners the median time to smear and culture conversion assessed by monthly spontaneous sputum samples was 33 days and 59 days, respectively. In that study, 4.2% of the patients had DR-PTB. Furthermore, Fitzwater et al.18 reported that for the 67 non-DR PTB patients in their study cohort, the median time to become culture-negative, assessed using weekly spontaneous sputum samples, was 37 days.
The present study has several important findings because, unlike previous studies, we evaluated the infectiousness of PTB patients using IS. The results of previous studies suggested that the average infectious period for smear-positive PTB was approximately 30 days28. However, as assessed by IS, 73%–81% of the patients with smear-positive PTB remained culture-positive after 4 weeks of anti-TB treatment. In addition, even in patients with smear-negative PTB, 76.9% remained culture-positive after 2 weeks of therapy, although almost all of them became culture negative after 4 weeks of therapy. Owing to the contribution of smear-negative PTB patients towards TB transmission, this unexpectedly long infectious period of smear-negative PTB is especially noteworthy.
There are several known factors associated with the likelihood that a PTB patient will infect others, including the extent and severity of disease, frequency of coughing, the quality, and volume of respiratory secretions, anti-TB therapy, and the characteristics of exposure4. Among these, cough is regarded as the predominant factor affecting PTB transmission and may be gradually decreased by chemotherapy3334. However, the direct measurement of the human-to-human transmission of PTB is complex and difficult35. Moreover, convincing data on the effectiveness of masks and cough hygiene in reducing PTB transmission are few, although they are widely used protection measures35. Therefore, microbiological criteria based on sputum analysis, such as conversion to culture-negative, have traditionally been used in clinical practice to determine PTB treatment success and infection control decisions34.
There are several limitations to this study. First, infectiousness is not determined only by the presence of viable MTB in respiratory specimens of PTB patients, and thus our results may not be generalizable. Although the presence of viable MTB in respiratory specimens is meaningful, cough and volume of respiratory secretion are also important modes of transmission, but these may be reduced after adequate therapy. Second, weekly IS in PTB cases is not common practice in clinical settings; therefore, our serial IS specimen based results may not be generalizable. In our institution, a separate, isolated single outpatient room for IS specimen collection has been available since March 2013. At that time, only one isolated negative-pressure room in ward was available since our institution was under construction for remodeling. Thus, it was needed to evaluate whether PTB patients required isolation as precaution against airborne transmission, especially from smear-positive PTB cases. In smear-negative PTB patients, we conducted IS before releasing them from isolation (after initiation of anti-TB medication), or when TB patients wanted to know their infectiousness status. Third, this study is a retrospective hospital patient-based study with a small sample size. Fourth, due to the retrospective nature, we cannot present results from more than 7 weeks after commencement of therapy. Moreover, we could not evaluate the relationship between negative culture conversion of IS and other factors known to affect infectiousness, such as the extent of disease or cavitation, due to the small sample size. Lastly, this study was not conducted under directly observed therapy, which may also have influenced the study results.
Despite these limitations, this study may be valuable, as it assessed negative smear and culture conversion duration based on not only serial IS but also using LM and SM. The accurate evaluation of infectiousness of PTB would not be easy in real world. So, we think and hope, this study may provide additional information and be helpful for PTB control.
In conclusion, our study demonstrates that the conversion time from culture positivity to culture negativity is longer than previously thought, even in patients with drug-susceptible PTB. Furthermore, many patients with smear-negative PTB, and of course patients with smear-positive PTB, remained culture-positive after 2 weeks of appropriate anti-TB therapy. Although further evaluation is needed, this long period of culture positivity in PTB has practical implications for TB control and will aid in optimizing the isolation period during anti-TB medication.
Acknowledgments
The authors thank Ms. Sula Kim for her help in data collection.
Notes
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.