Ethics in the Intensive Care Unit
Article information
Abstract
The intensive care unit (ICU) is the most common place to die. Also, ethical conflicts among stakeholders occur frequently in the ICU. Thus, ICU clinicians should be competent in all aspects for ethical decision-making. Major sources of conflicts are behavioral issues, such as verbal abuse or poor communication between physicians and nurses, and end-of-life care issues including a lack of respect for the patient's autonomy. The ethical conflicts are significantly associated with the job strain and burn-out syndrome of healthcare workers, and consequently, may threaten the quality of care. To improve the quality of care, handling ethical conflicts properly is emerging as a vital and more comprehensive area. The ICU physicians themselves need to be more sensitive to behavioral conflicts and enable shared decision making in end-of-life care. At the same time, the institutions and administrators should develop their processes to find and resolve common ethical problems in their ICUs.
Introduction
Physicians often experience ethical dilemmas in the clinical field. The intensive care unit (ICU) is the most common place of ethical conflicts, and many respiratory physicians face with these conflicts frequently. Recently, the intensive care dedicated system was implemented, and the critical care environment is rapidly changing in Korea. In this paper, we will describe the impact of ethical dilemmas on the quality of care and the role of the ICU physicians with respect to such dilemmas.
Impact of Ethical Conflicts in the ICU
Today's health care environment is increasingly complex. The complexity of technology-driven modern health care, value heterogeneity, individual rights, and the number of choices according to individual values are less conductive to good decision making1. Despite considerable technologic breakthroughs in the provision of intensive care medicine, mortality in the ICU remains high2 and ethical conflicts among stakeholders occur frequently in contemporary health care settings. These may have negative impacts on healthcare workers, patients, and their families, and lower the quality of intensive care.
In a previous study, over 70% of ICU workers reported perceived conflicts, which were often considered severe and were significantly associated with job strain3. Nurses perceived distressing situations more frequently than physicians did; additionally, 45% of the registered nurses surveyed reported having left or having considered leaving a position because of moral distress4. The ICU is one of the places in the hospital where family members suffer. More than two-thirds of family members visiting ICU patients have symptoms of anxiety or depression. In a French study, it was found that 75.5% of family members and 82.7% of spouses had symptoms of anxiety or depression in a multicenter study including 78 ICUs and 544 family members5.
Major Sources of Ethical Conflicts in the ICU
The incidence of ethical conflicts is higher in the ICU compared with the general wards. In a 3-year period during which a large urban teaching hospital had a total of 181,558 admissions, the hospital ethics committee staffed 0.16% of consultations. The services with the highest incidence of ethics committee consultations were the trauma ICU (0.88%) and medical ICU (0.56%)6. In another 1-year study, 4,968 patients were admitted to the adult ICUs at Columbia University Medical Center and 168 ethical consultations (3.3%) were requested 7. Although there are few reports on domestic data, according to a single center study by Park et al.8, the incidences of perceived conflicts that registered nurses reported during two different study periods were 2.1% and 0.5%, respectively.
Swetz et al.'s study9 showed the common diagnoses of cases referred to consultation at the Mayo Clinic in Rochester, Minnesota, during a 10-year period, including malignancy (18%) and neurologic disease (18%), followed by cardiovascular disease (17%), multi-organ failure (11%), pulmonary disease (9%), and others. According to Romano et al.'s study7, the most common diagnosis was cardiovascular disease, followed by neurologic disease, pulmonary disease, renal disease, gastrointestinal disease, malignancy, multi-organ system failure, psychiatric disease, developmental or genetic disease, and miscellaneous.
The 1-day cross-sectional questionnaire survey from 397 ICUs in 29 countries showed that conflicts were perceived by 5,268 respondents (71.6%) and that nurse-physician conflicts were the most common (32.6%)3. The major sources of conflicts in ICUs were behavior-related conflicts and conflicts associated with end-of-life (EOL) care. The most common conflict-causing behaviors were personal animosity, mistrust, and communication gaps. During EOL care, the main sources of perceived conflict were a lack of psychological support, absence of staff meetings, and problems with the decision-making process.
In particular, verbal abuse was one of the conflict-causing behaviors, and nurse-physician disruptive behavior was found to have a negative impact on patient safety10. As Sofield and Salmond's study reported11, 51% of respondents reported patient errors occurred as a result of such behavior. The most common forms of verbal abuse and/or disruptive behavior was condescending language. Other common types of disruptive behavior included disrespect and a failure to return phone calls12131415. In many studies, between 17% and 41.9% of healthcare providers reported a specific adverse event that occurred as a result of disruptive behavior1617. As a result, eleven recommendations have been made by The Joint Commission to help organizations implement the group's standards (Table 1)18.
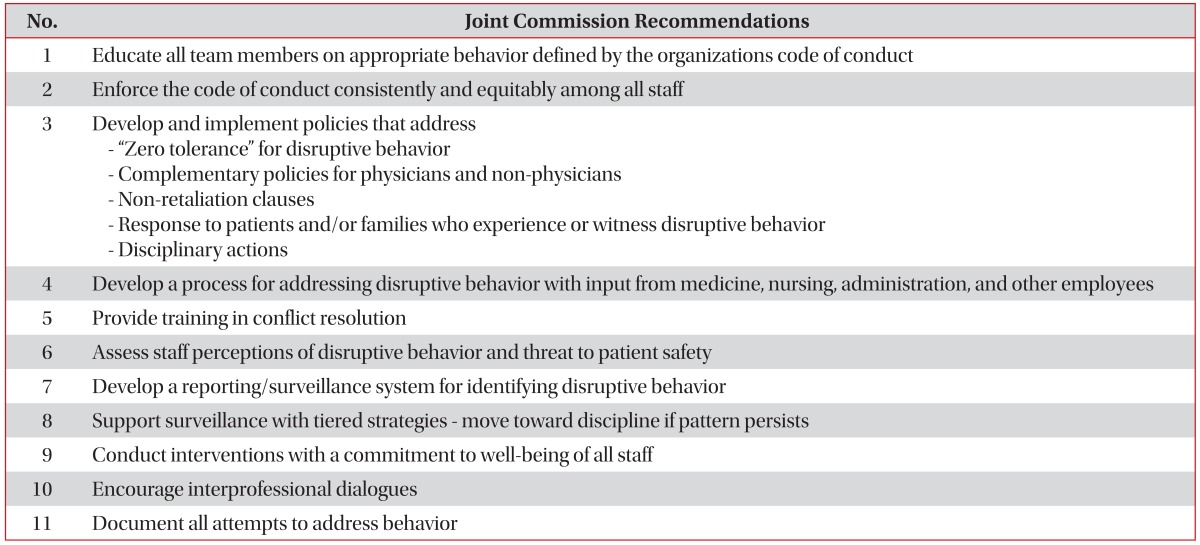
The Joint Commission Recommendations for managing disruptive behavior
Burnout Syndrome and Moral Distress of Health Care Professionals
ICU caregivers work in a stressful environment, which can lead to burnout syndrome19. In addition, the ethical environment of their unit and ethical conflicts cause moral distress, which is believed to be associated with burnout.
It is well known that burnout can affect up to 45% of ICU nurses and physicians2021. Burnout is a psychological syndrome that occurs in response to chronic emotional and interpersonal stressors at work. It can lead to emotional instability, commitment difficulties, a feeling of failure, and an urge to leave one's job. Consequences to caregivers' health include insomnia, irritability, and depressive symptoms, which in turn can impact the quality of the care they provide2022. Burnout in physicians tends to manifest as the provider caring less for his or her patients, and the number of medical errors increases2223.
The Maslach Burnout Inventory, which measured the burnout of the nurses who work in Korean university hospitals, demonstrated significant emotional exhaustion and high-burnout conditions in that professional environment and profession2425.
In Canada, it was found that internal medicine residents value the opportunity to learn from dying patients, but often lack supervision and then experience emotional distress26. The majority of respondents agreed the learning experience gained from providing EOL care was meaningful, although 48.1% felt guilty and 40.6% felt failure at least some point after a patient's death. A domestic single center study reported that 69.1% of residents encountered serious ethical dilemmas at least once a year, but the majority of these residents claimed to have resolved those dilemmas either alone or through discussions with colleagues without an attending physician's advice27.
The high rate of physician suicide is also well known; the suicide rate among male doctors is 40% higher than among men in general, whereas the rate among female doctors is 130% higher than among women in general28. Health care professionals are frequently exposed to emotional stress and exhaustion.
Type of Ethical Problems and Education in Ethics
When we examine the behavior of the health professionals involved, it can be seen that different types of moral behavior can give rise to these problem. Types of ethical problems are presented in Table 229.
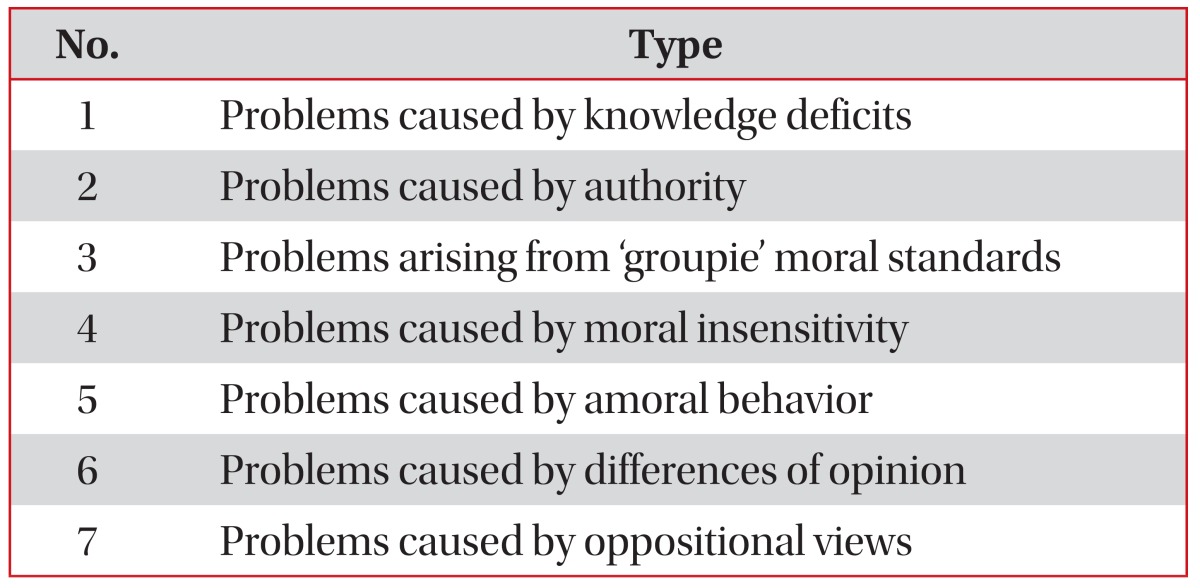
Various types of moral behavior of health professionals
A lack of knowledge or education in health ethics is a common cause of ethical dilemmas occurring in ICU. This manifests when the health professional does not see a situation as being an ethical or moral problem. An example is do not resuscitate (DNR) orders on chronically ill patients. The problems arising from knowledge deficits could decrease considerably if professionals receive training or education in recognizing the associated moral problems and how to be competent in moral standards of care29. This is the reason why education in ethics is important.
Doctors' and patients' values sometimes differ, and even though medical decision making is complex, it should be approached using the principles of bioethics. Such ethical decision making training in the clinic would make patients' best interests and health professionals' values consistent with the fundamental values of our society.
Ethical Issues of EOL Care in the ICU
During EOL care, the main cause of ethical conflict was found to be the inappropriateness of care, including a lack of psychological support and problems with the decisionmaking process. In Korea, most terminal cancer patients die in medical institutions. However, the quality of EOL care in Korean ICUs does not ensure the terminally ill patient's autonomy and dignity at the end of the patient's life.
One of the most important EOL issues is how health care professionals communicate the patients' prognoses to them3031. Accurate prognostic information helps patients and physicians make sound medical decisions and care choices 3132. Yun et al.'s study31 found that patients who learned their prognoses from their physicians had better outcomes, such as lower rates of emotional distress and a higher health-related quality of life (QOL), but a substantial proportion of patients did not receive such information from their physicians. Despite the fact that most patients are resistant to chemotherapy regardless of cancer type near the EOL, chemotherapy was still frequently administered in Korea33. However, a multicenter prospective cohort study of patients with cancer entering the terminal stage of their disease shows that the patients' awareness of terminal illness, use of palliative care, and admission to an ICU do not influence the survival of terminally ill patients34.
Surrogate decision-making was frequently observed among Korean cancer patients, especially when the patient's death was imminent, and for decisions related to EOL care. The proportion of patient self-determination for DNR directives was extremely rare near the EOL period, far from an ethical ideal35. Annually, thousands of terminal cancer patients still die under cardio-pulmonary resuscitation in Korean ICUs. Among nurses and physicians who work in adults ICUs in Europe, perceptions of inappropriate care have been frequently reported. The main reported reason for perceived inappropriateness of care was a mismatch between the level of care and the expected patient outcome, usually in the direction of perceived excess intensity of care36.
Despite all the literature, there is little discussion about the QOL of terminal cancer patients in their end-stages of life or the optimal triage of admission to an ICU. According to US Medicare database, from 1993 to 2002, an increasing proportion of patients who had been diagnosed with advanced lung cancer received ICU care near the end of their lives. Twothirds of patients died either during or within 1 month of hospitalization 37. Hwang et al.'s study38 showed that ICU mortality and in-hospital mortality rates of patients with lung cancer admitted to the medical ICU were 53.6 and 61.8%, respectively; very poor values.
Shared Decision Making
The ICU is not the adequate place for the care of terminally ill patients because it is not designed for EOL care. If the disease state of the patient is not curable, how can we determine the best treatment goals for the patient? The physician used to be the best situated to make decisions reflecting the patient's best interests. However, it is no longer appropriate to assume a concordance between physician and patient values. Under the shared decision-making model, physicians work together with patients and their families to define the patient's healthcare values, beliefs, and treatment preferences. The physician not only provides information about treatments but also recommends the treatments he or she believes to be most concordant with the patient's values and goals39.
The Role of ICU Professionals
There are many barriers to overcome ethical dilemmas in different cultures. ICU leaders or dedicated professionals have the responsibility to find and resolve the 'hidden' barriers which cause conflicts and lead to a decline in the quality of care in their respective units.
In order to do that, it is important to make a constant effort to communicate with colleagues, as well as with patients and their families. At the same time, ethics training programs for residents, critical care nurses, and fellows are necessary and should be administered in their hospital and ICU trainings.
Multiple recent studies have documented that clinical practices such as educational interventions, family conferences, and the introduction of protocols might be necessary to resolve conflicts and to improve the quality of care40.
Conclusion
Physicians frequently confront ethical issues in clinical practice, especially in the ICU. However experience, common sense, and simply being a good person, do not guarantee that physicians can identify or resolve ethical dilemmas41.
Good clinical decision-making is only possible when the medical decision-making and ethical decision-making are correctly balanced. Knowledge about common ethical dilemmas and training in ethical decision-making is essential. At the same time, the ICU leaders and hospital directors should prepare protocols to find and resolve the common ethical problems in their hospital.
Notes
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.