


Introduction
Idiopathic pulmonary fibrosis (IPF) is an inflammatory fibrotic lung disease of unknown etiology. Unfortunately, IPF is a progressive and irreversible disorder. In general, median survival of IPF patients is 2.5 to 5 years with or without treatment1,2. The pathogenesis of IPF is poorly understood3. One of the major advances in the pathogenesis of IPF is the shift in current paradigms from inflammation to abnormal wound healing4. In the wound healing process, coagulation cascade is activated locally from tissue factor dependent extrinsic pathway5. Recent studies implicated protease-activated receptor-2 (PAR-2) in the fibrosis.
PAR-2 is a G-coupled 7-transmembrane receptor that is activated by tethered peptide ligand, which is exposed after enzymatic cleavage of the specific site in the extracellular N-terminal6. PAR-2 is expressed in various tissues and abundant in kidney, pancreas, and gastrointestinal tissue than in heart and lungs7. In each organ, PAR-2 expressions were mainly located in endothelial and epithelial cells8. Recent studies suggested association of PAR-2 activation with airway inflammation9-11 and pulmonary fibrosis12. In addition, up-regulation of PAR-2 was observed in lung tissue of IPF patients and possible pathway of the development of pulmonary fibrosis13. Recently we conducted PAR-2 expression of surgical specimen from IPF patients, and we found the possibility of the association between PAR-2 expression and clinical outcome of IPF14. So the aim of this study was to evaluate the overexpression of PAR-2 in inflammatory cells from peripheral blood and bronchoalveolar lavage fluid in IPF patients.
Materials and Methods
1. Study population
We included the patients with IPF in Seoul National University between May 2011 and March 2012. The diagnosis of IPF was based on the established criteria (20) and clinical diagnosis was judged according to international guidelines. Peripheral blood and bronchoalveolar lavage fluid were collected after informed consent. The protocol was approved by the Institutional Review Board of the Seoul National University Hospital. All patients gave written informed consent. The study was conducted in accordance with the Declaration of Helsinki.
2. Mononuclear cell isolation
Blood (5 mL) was drawn into heparinized tubes and mononuclear cell isolation was performed within 6 hours from acquisition of specimen. Blood was diluted phosphate buffered saline with equal volume. The mixture was layered over 5 mL Ficoll-Paque-Plus solution (density 1.077/mL; Amersham Biosciences, Uppsala, Sweden). The layers of density gradient were separated after centrifugation (2,100 rpm for 20 minutes). Mononuclear cells were harvested with micropipette.
3. Flow cytometry
Mononuclear cells (1.0├Ś106/mL) were fixed in 4% paraformaldehyde for 20 minutes at 4Ōäā and then incubated 30 minutes room temperature with CD3 (BD Biosciences, San Jose, CA, USA), CD14 (BD Biosciences), PAR-2 (Santa Cruz Biotechnology, Santa Cruz, CA, USA). Each isotype controls were used for calibration.
4. Reverse transcription polymerase chain reaction (RT-PCR) and PCR
The total RNA was extracted from the mononuclear cells using RNeasy Mini kit (Qiagen, Valencia, CA, USA), and PCR was followed using commercially available kit (Bioneer, Daejeon, Korea), according to manufacturere's instructions. Oligonucleotide primers (forward: 5'-GTT GAT GGC ACA TCC CAC GTC-3', reverse: 5'-GTA CAG GGC ATA GAC ATG GC-3') were designed for PAR-2. The PCR conditions were as follows; a pre-denaturating for 94Ōäā for 1 minute, followed by 40 cycles fo denaturation at 94Ōäā for 1 minute, annealing at 64Ōäā for 1 minute, and extension at 72Ōäā for 1 minute. PCR products were separated by electrophoresis through 1% agarose gel and the signal intensity was analyzed by ImageJ. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) controls were used to standardize the quantification of samples.
RT-PCR was conducted to examination the mRNA expression of PAR-2 and GAPDH.
Results
1. Study population
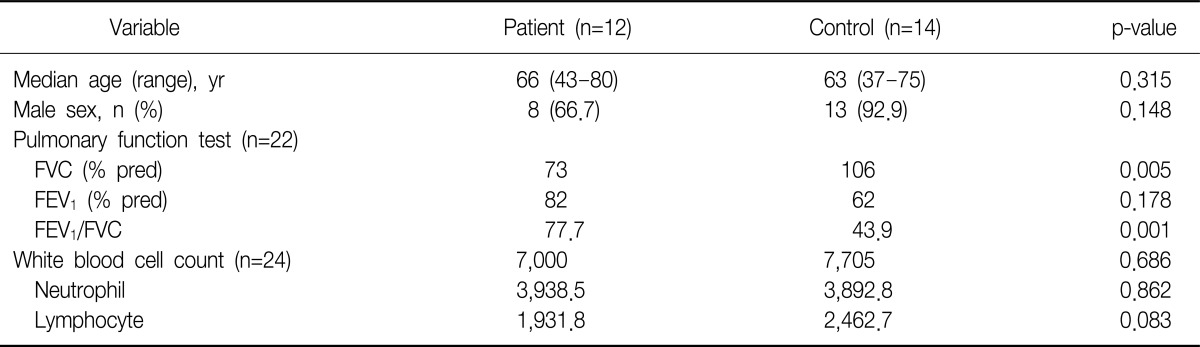
Table 1 shows the clinical characteristics of IPF patients (n=12) and controls (n=14). Median age was 66 in IPF group and 63 control group. Pulmonary function test showed statistically significant different forced vital capacity (FVC) and forced expiratory volume in one second/FVC, because chronic obstructive pulmonary disease (COPD) patients (n=8) were included in control group.
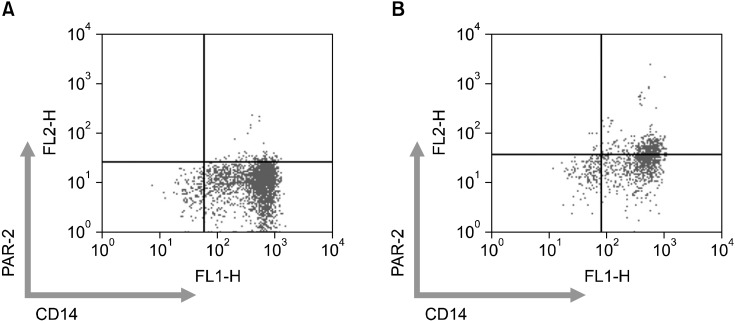
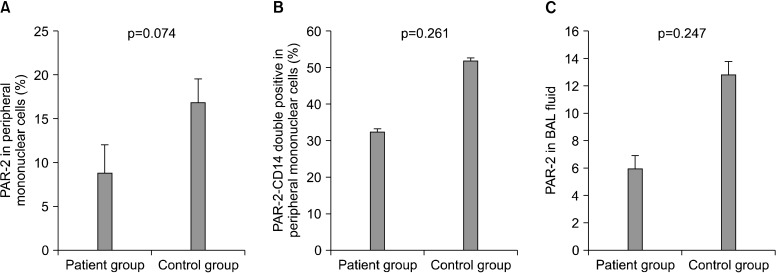
2. PAR-2 receptor expression in flow cytometry
We conducted flow cytometry analysis from 26 peripheral blood (patient group, 11; control group, 13) and 7 bronchoalveolar lavage (BAL) fluid (patient group, 5; control group, 2) (Figure 1). CD3, CD14, CD20, PAR-2 expression were analyzed. PAR-2 expression was not significant different between patient and control group in peripheral blood and BAL fluid (Figure 2). The proportion of PAR-2 and CD14 double positive among CD14 single positive was no different in both groups (p=0.247).
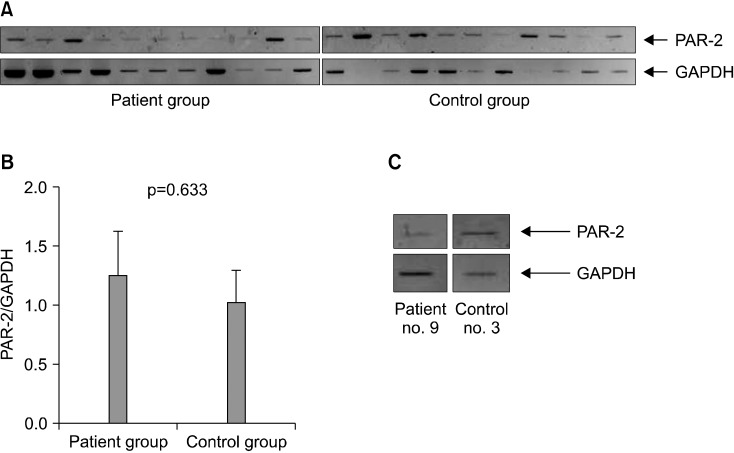
3. PAR-2 mRNA expression
Among 26 persons, PAR-2 mRNA assessment was performed in 19 persons (patient group, 10; control group, 9). mRNA expression of PAR-2 was not different between patient and control group (p=0.633) (Figure 3). Because there was paucity of cellularity in BAL fluid, only two cases (patient, 1; control, 1) were conducted RT-PCR for mRNA expression of PAR-2.
Discussion
The understanding of IPF pathogenesis has shifted from inflammatory response to aberrant wound healing of unknown etiology4. In other words, the pulmonary fibrosis is considered as the common end pathway of aberrant wound healing. Interestingly, during the fibrotic process, coagulation cascade activation was frequently observed not only IPF but also other inflammatory conditions such as systemic sclerosis and acute respiratory distress syndrome15-17. In acute lung injury animal model, uncontrolled activation of coagulation cascade and pulmonary fibrosis was also observed, and furthermore PAR-2 activated by Factor Xa was a significant receptor for the development of pulmonary fibrosis12. These findings suggest the possible role of PAR-2 in the pathogenesis or progression of pulmonary fibrosis.
As described above, we reported the relationship between immunohistochemical expression of PAR-2 and worse clinical outcomes of IPF patients14. But this study did not show an increased PAR-2 receptor expression in BAL fluid and peripheral mononuclear cells with IPF patients. The relationship between activation of coagulation cascade and pathogenesis of IPF might be irrelevant. Moreover, warfarin did not show a beneficial effect in progressive IPF in recent study18. In addition, this study had some limitations. Most of all, study population was so small. We included only 12 IPF patients during 10 months. The second, control group was not homogeneous. Among 14 control group, 8 were COPD patients. COPD is well known systemic inflammatory disease and PAR-2 is associated with inflammation19. So it is explainable that PAR-2 receptor expression was increased in control group (Figure 3).
In conclusion, PAR-2 receptor and mRNA expression was not increased in IPF patients compared to control group.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






