


Introduction
In Korea, there were 492 cases of malignancies in the mediastinum in 20111. The incidence of thymic carcinoma is less than 50 per year. Among the thymic carcinoma, only three cases of primary thymic adenocarcinoma have been reported in Korea for now.
Thymic carcinoma originated from thymic epithelium with a high degree of histological anaplasia, cell atypia, paucity of lymphocytes, and increased proliferation2. Most common subtypes of thymic carcinoma based on their histological differentiation is keratinizing/non-keratinizing squamous cell carcinoma (76%) followed by basaloid type (3%)3. Neuroendocrine, mucoepidermoid, lymphoepithelioma-like, sarcomatoid, clear cell, papillary and anaplastic subgroups are also reported4. Among those subtypes of thymic carcinoma, primary thymic adenocarcinoma is a very rare subtype of thymic carcinoma. Subtypes of primary thymic adenocarcinoma are listed below; mucinous, papillotubular, conventional, papillary, and not otherwise specific (NOS)5.
More than half of the thymic carcinoma showed overexpression of c-kit, a type III tyrosine kinase receptor protein encoded by the proto-oncogene kit which regulates cell proliferation, differentiation, adhesion and apoptosis (50%-80%) while thymoma rarely presented c-kit expression (0%-5%)6. Malignant transformation of benign epithelial cells of thymic cyst is necessary for making a diagnosis of the primary thymic adenocarcinoma. Clear-cut atypia of tumor epithelial cells with the severity typical of carcinoma with exclusions of carcinoids, metastasis to the thymus, germ cell tumor, and mesenchymal tumors with epithelial features are major criteria of the thymic carcinoma7. Immunohistochemical (IHC) staining of CD5 (leukocyte marker expressed on differentiating thymocytes) is useful in differentiating thymic from non-thymic carcinomas8. Negative IHC results in thyroid transcription factor 1 (TTF1) and calretinin are also important to exclude those tumors derived from the lung and pleura from the primary thymic adenocarcinoma5.
For the diagnosis of the primary thymic adenocarcinoma, radiologic findings confirming the anterior mediastinal mass with no evidence of primary tumor in other organs and pathologic diagnosis based on hematoxylin and eosin (H&E) staining and IHC staining are required.
For the clnical presentation of the thymic carcinoma, the most common symptoms are chest pain, shortness of breath, cough, hoarseness of the voice, dysphagia those derived by pressure effect of the mass4. About 41% of the patients with thymic adenocarcinoma nearly present any symptoms5.
Because of the rareness of the cases, standard treatment for the primary thymic adenocarcinoma has not been established so far resulted in poor clinical outcomes. For the more information about the primary thymic adenocarcinoma, we underwent literature review of the almost all previously published case reports and small case series in our knowledge except one case written in Chinese which will be discussed later. We report a case of rare primary thymic adenocarcinoma which is carried out in accordance with the Declaration of Helsinki and Korean Good Clinical Practice (GCP) guidelines with the informed consent of the patient. The review of the study is approved by the respective Institutional Review Board (IRB) of the Gangnam Severance Hospital (IRB No. 3-2014-0194).
Case Report
A 36-year-old man presented with hoarseness for 3 months and infiltrative mass in the left upper mediastinum on neck computed tomography (CT) scan. He visited our hospital via local otolaryngology-head and neck surgery clinic after the diagnosis of upper respiratory tract infection treated with cold medicine for a while. The patient presented no medical history except a 23 pack-year smoking history. On the physical examination, neither engorged neck vein nor palpable neck nodes were observed.
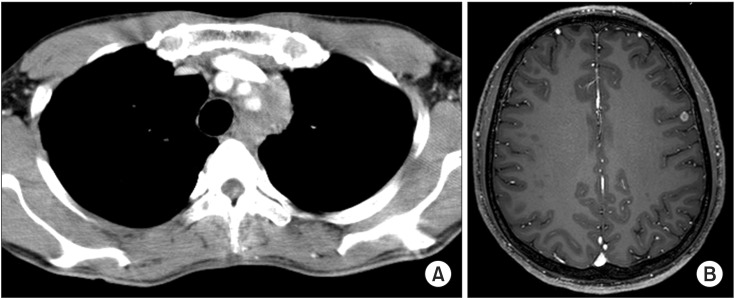
Initial chest CT scan (Figure 1A) showed an infiltrative mass in the left upper mediastinum (4.1├Ś3.1├Ś5.4 cm), encircling the left common carotid artery and left subclavian artery. Brain magnetic resonance imaging (MRI) with contrast (Figure 2B) revealed focal enhancing lesion in the left frontal lobe suggesting metastasis. Torso positron emission tomography (PET)/CT presented about 1.6-cm hypermetabolic lesion in left paravertebral region of thoracic spine two (T2) level and 3.9-cm-sized hypermetabolic mass in the left upper mediastinal region just above the aortic arch which seems the same lesion observed with chest CT. Those radiologic imaging study were suggestive small cell lung cancer. Elevated plasma levels of carcinoembryonic antigen (CEA) and neuron specific enolase (NSE) were also supportive evidence for suggesting small cell lung cancer (CEA, 6.0 ng/mL [0.2-5.0 ng/mL]; NSE, 12.9 ng/mL [7.5-12.5 ng/mL]). However, thoracoscopic biopsy of the mediastinal mass showed unexpected results at all; presence of carcinoma suggestive of adenocarcinoma was reported. To conclude this finding, multiple mediastinoscopic biopsies of the left upper mediastinal side of the infiltrative mass and lymph nodes around the mass were performed. Pathologic results showed an adenomatous feature with glandular formation and immunoreactive for cytokeratin, CEA, and CD5 (Figure 2A, B) which means this tumor is adenocarcinoma originated from the thymus. IHC staining for TTF1 and napsin A (Figure 2C) were negative and was able to exclude tumors derived from the lung. The patient diagnosed as primary thymic adenocarcinoma (conventional subtype) and staged as Masaoka stage IV. A complete resection was not performed due to the invasion of the proximal vessel and aortic arch.
After the pathologic diagnosis has confirmed, the patient underwent four cycles of chemotherapy composed of 120 mg/m2 etoposide for D1-3 and 60 mg/m2 cisplatin for a D1 every 3 weeks. Concomitant radiation therapy (6,000 cGy/30 fractions; Tomo-Helical, TomoTherapy, Wisconsin MI, USA) to the lesion followed by salvage radiotherapy to the metastatic brain lesion (4,200 cGy/12 fractions; Tomo-Helical) and mediastinum (3,000 cGy/12 fractions; Tomo-Helical) were also administrated. The patient completed the planned treatment without other complications.
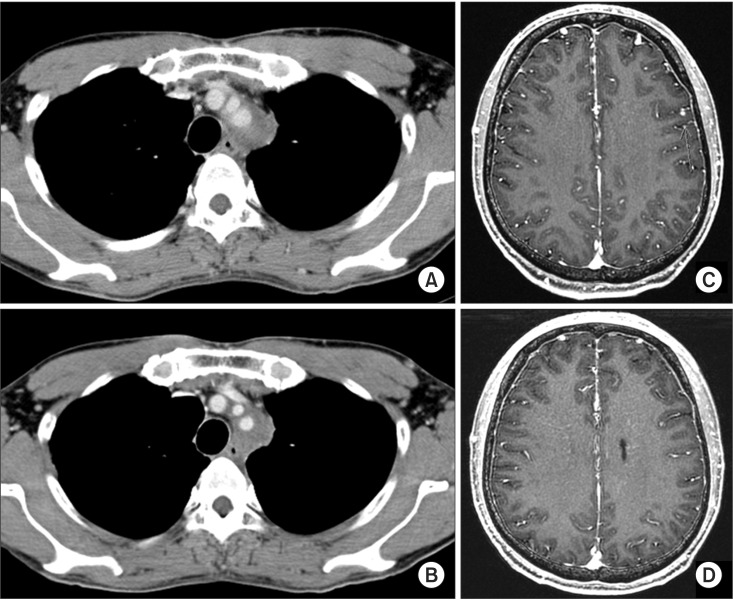
Chest CT scan performed at a 1-month follow-up visit (Figure 3A) revealed decreased mass size (4.1 cm to 2.8 cm in diameter) and 3-month follow-up chest CT (Figure 3B) presented stable disease status described as no interval change of residual encasing solid mass lesion at the left superior mediastinum near the proximal neck vessel and aortic arch. Brain MRI performed at a 1-month follow-up visit (Figure 3C) and 3-month follow-up visit (Figure 3D) presented decreased focal lesion on left frontal lobe area. PET-CT taken at 1-month follow up visit showed disappeared hypermetabolic mass lesion just above the aortic arch, nearly disappeared hypermetabolic nodes in left supraclavicular region and markedly decreased fluoro-2-deoxyglucose uptake in the shrunken lesion of left paravertebral region, second thoracic spine level which are considered favorable response to the treatment. Regular chest CT follow-up in 3 months is planned.
Discussion
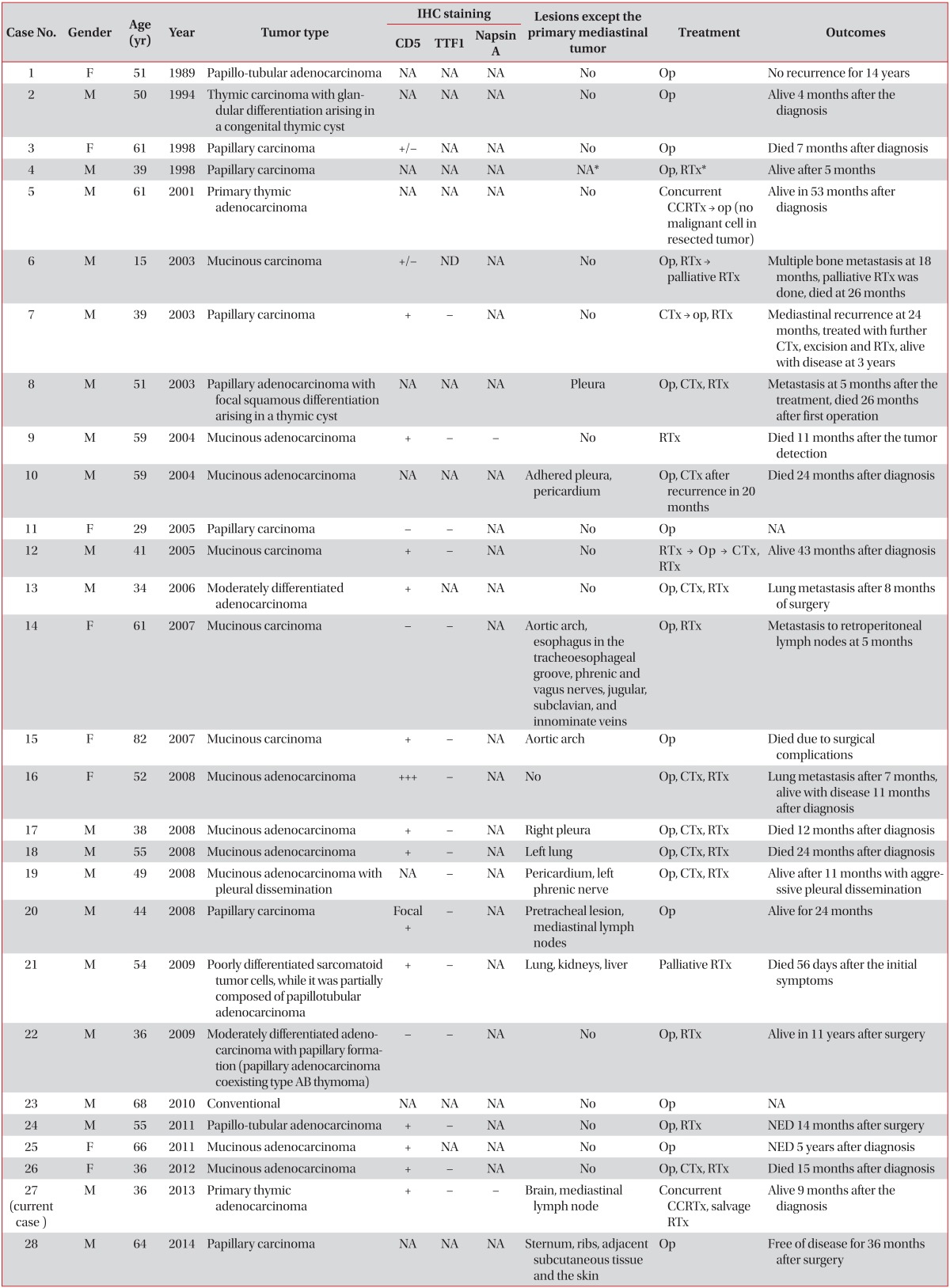
Primary thymic adenocarcinoma is an extremely rare disease especially in female. Since the first case report from the japan in 1989 by Moriyama et al. (Table 1, case No. 1)5, twenty-seven cases of primary thymic adenocarcinoma have been reported. Literature review on primary thymic adenocarcinoma is shown in Tables 1 and 2. In Table 1, we analyzed a total of 28 cases including our case to the literally reviewed data. Patient range in age was from 15 to 82 years and the median age was 51 years. Twenty out of 28 was male and male:female ratio is 2.5:1.
Fifteen out of 28 patients were immunoreactive for CD5 which is a leukocyte marker expressed during a differentiation of thymocyte. Nine out of 28 were not available to find out a record for IHC staining of CD5. Sixteen out of 28 were tested for TTF1 and presented negative value which means those lesions are not come from the lung adenocarcimona. Except our case, only one case reported in 2004 underwent Napsin A IHC staining and presented negative value (Table 1, case No. 9).
There were variable lesions except the primary mediastinal tumor; pleura, pericardium, aortic arch, mediastinal lymph node, sternum, lung, and extrathoracic lesion like liver, kidneys, and brain.
For the clinicopathological analysis described in Table 2, 12 patients presented thymic mucinous adenocarcinoma accounting the most common subtype of the thymic adenocarcinoma followed by papillary carcinoma presented in eight patients. Three out of 28 showed papillotubular adenocarcinoma. Three out of 28 were conventional and 2 out of 28 were classified NOS. Male patients tended to present more lesions except the primary mediastinal tumor than female cases (male vs. female is 9 out of 20 vs. 2 out of 8) (Table 2).
Most primary thymic adenocarcinoma cases reported to date were operable as noted in Table 1. Those cases underwent operation followed by postoperative radiotherapy alone or postoperative chemotherapy plus radiotherapy to the resected lesion. So far, the outcomes of primary thymic adenocarcinoma treated with resection of the tumor followed by radiotherapy alone were not successful. Bone metastasis at 18 months (Table 1, case No. 6) and retroperitoneal lymph node metastasis at 5 months (Table 1, case No. 14) were reported in those cases. Postoperative chemotherapy plus radiation therapy expected to favorable outcomes-but most of the cases revealed metastasis and death of disease at 11 to 26 months (Table 1, case Nos. 8, 13, 17, 18, 19, 26). Although there was one 41-year-old man case presented no evidence of disease at 43 months after diagnosis got radiotherapy to the primary thymic mucinous adenocarcinoma lesion followed by resection both of the primary thymic adenocarcinoma (10.5├Ś8.0├Ś2.5 cm) and metastatic lung lesion with adjuvant radiotherapy and chemotherapy (Table 1, case No. 12), one 82-year-old female case passed away from the complication of surgery after resection of 14.5├Ś7.0-cm-sized mass (Table 1, case No. 15).
Comparing with other cases, we described a 36-year-old male patient presenting inoperable primary thymic adenocarcinoma with infiltration to the proximal pulmonary vessels and aortic arch. He was rather young considering the median age (51 years old) of the literally reviewed cases. He showed metastatic brain lesion and staged as Masaoka stage IV. Tumor tissue underwent IHC staining for CD5, TTF1, and Napsin A. TTF1 and Napsin A are distinguishable point of our case from previously reported cases. TTF1 and Napsin A are well known IHC markers to differentiate primary lung adenocarcinoma from squamous carcinoma13. Napsin A is reported to present 100% specificity and 81% sensitivity to detect adenocarcinoma which negative predictive value is 83%. TTF1 showed 98% specificity and 70% sensitivity and 79% of negative predictive value. Those scores are reported as most valuable among the other similar IHC markers13.
He underwent four cycles of cisplatin and etoposide with concurrent radiotherapy to the lesion and salvage radiotherapy to the brain resulted in favorable clinical outcome. Follow-up chest CT and brain MRI at 1 month and 3 months after the treatment showed stable disease status without symptoms. There is no standard treatment for inoperable primary thymic adenocarcinoma. For the operable thymic carcinoma which may include adenocarcinoma of the thymus origin, surgical resection with adjuvant radiotherapy and/or adjuvant cisplatin-based chemotherapy is recommended3. Although the subtypes of the tumor were not the primary thymic adenocarcinoma, seven inoperable thymoma or thymic carcinoma with extra-thoracic site lesions like supraclavicular lymph node metastasis treated with palliative chemotherapy for the initial treatment and concluded the presence of extrathoracic metastasis and histologically diagnosed as a thymic carcinoma are significant factors for progression free survival (hazard ratio, 6.62; 95% confidence interval, 1.19-24.17, p=0.004)14. In our case, we applied concurrent chemoradiation therapy to the primary thymic adenocarcinoma patient with extrathoracic metastasis like brain metastasis (masaoka stage IVb) showed favorable clinical outcome.
Considering listed above, we conclude that it is reasonable underwent IHC staining for CD5, TTF1, and Napsin A for the cases suggesting primary thymic adenocarcinoma on the H&E staining. Furthermore, when the case is inoprerable primary thymic adenocarcinoma with extrathoracic metastasis, concurrent chemoradiation therapy with focal salvage radiotherapy could be an efficient treatment option for favorable clinical outcome.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






