Clinical Characteristics and Changes of Clinical Features in Patients with Asthma-COPD Overlap in Korea according to Different Diagnostic Criteria
Article information

Abstract
Background
Asthma–chronic obstructive pulmonary disease (COPD) overlap (ACO) is a condition characterized by the overlapping clinical features of asthma and COPD. To evaluate the appropriateness of different sets of ACO definition, we compared the clinical characteristics of the previously defined diagnostic criteria and the specialist opinion in this study.
Methods
Patients enrolled in the KOrea COpd Subgroup Study (KOCOSS) were evaluated. Based on the questionnaire data, the patients were categorized into the ACO and non-ACO COPD groups according to the four sets of the diagnostic criteria.
Results
In total 1,475 patients evaluated: 202 of 1,475 (13.6%), 32 of 1,475 (2.2%), 178 of 1,113 (16.0%), and 305 of 1,250 (24.4%) were categorized as ACO according to the modified Spanish Society of Pneumonology and Thoracic Surgery (SEPAR), American Thoracic Society (ATS) Roundtable, Global Initiative for Asthma (GINA)/Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria, and the specialists diagnosis, respectively. The ACO group defined according to the GINA/GOLD criteria showed significantly higher St. George's Respiratory Questionnaire and COPD Assessment Test scores than the non-ACO COPD group. When the modified SEPAR definition was applied, the ACO group showed a significantly larger decrease in the forced expiratory volume in 1 second (FEV1, %). The ACO group defined by the ATS Roundtable showed significantly larger decrease in the forced vital capacity values compared to the non-ACO COPD group (–18.9% vs. –2.2%, p=0.007 and –412 mL vs. –17 mL, p=0.036). The ACO group diagnosed by the specialists showed a significantly larger decrease in the FEV1 (%) compared to the non-ACO group (–5.4% vs. –0.2%, p=0.003).
Conclusion
In this study, the prevalence and clinical characteristics of ACO varied depending on the diagnostic criteria applied. With the criteria which are relatively easy to use, defining ACO by the specialists diagnosis may be more practical in clinical applications.
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are the most common obstructive lung diseases, although they have different underlying pathophysiology and clinical manifestations [1]. Nevertheless, some patients show clinical features of both asthma and COPD [2]. Asthma-COPD overlap (ACO) is a condition characterized by overlapping clinical features of asthma and COPD. There is no consensus definition for ACO; several definitions have been proposed to categorize patients with features of both asthma and COPD. The most widely used diagnostic criteria are those of the American Thoracic Society (ATS) Roundtable [3], the Spanish Society of Pneumonology and Thoracic Surgery (SEPAR) [4], and the Global Initiative for Asthma (GINA)/Global Initiative for Chronic Obstructive Lung Disease (GOLD) [5]. Since there is currently no gold standard test to diagnosed asthma, the clinical opinion of an experienced clinician is essential [6]. Thus diagnosis of ACO by a specialist clinician is also important. However, the appropriateness of these criteria may differ according to the ethnic, cultural, linguistic and clinical characteristics of each country. Several Korean studies have evaluated the clinical characteristics of ACO patients [7,8]. However, further longitudinal studies are necessary, since the clinical characteristics and prognosis of ACO vary depending on the criteria used. Some studies have reported that ACO shows a more rapid decline in lung function [9,10], although another study reported otherwise [7]. Additional clinical data on changes in symptom and pulmonary function test scores in ACO patients are necessary.
This retrospective study applied four sets of ACO diagnostic criteria to a cohort of Korean COPD patients. We compared clinical presentations and appropriateness of the different sets of criteria so as to know which criteria is most applicable in Korean ACO population.
Materials and Methods
1. Diagnostic criteria for ACO
The following diagnostic criteria for ACO were applied: (1) the ATS Roundtable criteria [3], (2) the modified SEPAR criteria proposed by Soler-Cataluna et al. [4], (3) the GINA/GOLD criteria [5], and (4) specialist diagnosis based on own experience and beliefs (clinician’s diagnosis). The criteria are detailed in Supplementary Table S1.
2. Data collection
Patients enrolled in the KOrea COpd Subgroup Study (KOCOSS) were recruited from 48 tertiary referral hospitals in Korea, and were required to regularly visit the hospital so that their COPD status could be tracked via self-administered questionnaires, and to undergo pulmonary function tests at least every 6 months [11]. All data were checked for validity and coherence before evaluation. The inclusion criteria were as follows: aged ≥40 years and post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio <0.7.
This retrospective cohort study was initiated by the Asthma Study Group of the Korean Academy of Tuberculosis and Respiratory Disease. Questionnaires were administered between July and October 2016, and the results were analyzed together with the baseline KOCOSS data. Based on the questionnaire data, patients were categorized into ACO and non-ACO COPD groups according to the four sets of diagnostic criteria detailed above.
3. Statistical analysis
Statistical analyses were performed using SPSS software version 20.0 (IBM Corp., Armonk, NY, USA). Continuous data are expressed as the mean and range. Categorical variables were compared between the ACO and non-ACO COPD groups using the chi-squared test, and continuous variables were analyzed using Student’s t test or the Mann-Whitney U test, depending on the normality of the data distribution. To evaluate changes in FEV1 and FVC over 3 years, mean delta values (difference between year 3 and baseline values) were compared between the ACO and non-ACO COPD groups using the independent t test. The paired t test was also used to analyze within-group changes in continuous variables. A p<0.05 was considered significant in all analyses.
4. Ethics statement
Written informed consent was obtained from all patients enrolled in this study. Ethical approval was obtained from the ethics committees of each participating medical center.
Results
1. Prevalence of ACO
In total 1,475 patients evaluated: 202 of 1,475 (13.6%), 32 of 1,475 (2.2%), and 178 of 1,113 (16.0%) were categorized as ACO according to the modified SEPAR, ATS Roundtable, and GINA/GOLD criteria, respectively. Furthermore, 305 of 1,250 patients (24.4%) were categorized as ACO according to specialist diagnosis. The proportions of patients who did and did not satisfy the various diagnostic criteria for ACO are shown in Table 1. Regarding the modified SEPAR criteria, 87 patients met the major criteria and 125 patients met the minor criteria. Regarding the major criteria, 5.5% of the patients showed a bronchodilator response (BDR) >15%/400 mL. Regarding the minor criteria, 58.2% of the patients showed an IgE level >100 IU or a history of atopy, and 11.8% showed a BDR >12%/200 mL on at least two separate occasions. In terms of blood eosinophils, 17.0% of the patients showed a baseline eosinophil count >5%. Regarding the ATS Roundtable criteria, 66 patients met the major criteria and 347 met the minor criteria. Regarding the major criteria, 80.2% of the patients had a smoking history of ≥10 pack-years, and 5.6% showed a BDR >400 mL (FEV1). Regarding the minor criteria, 8.1% of the patients had a history of atopy or allergic rhinitis, 11.8% had two separate BDRs of ≥12%/200 mL, and 21.7% showed eosinophil counts ≥300 cells/μL. Regarding the GINA/GOLD criteria, among 1,099 patients who responded to the asthma questionnaire, 17.2% responded positively to three or more asthma questions and 96.2% responded positively to three or more COPD questions. The number of patients who responded positively to a minimum of three questions for both asthma and COPD was 176 (16.0%).
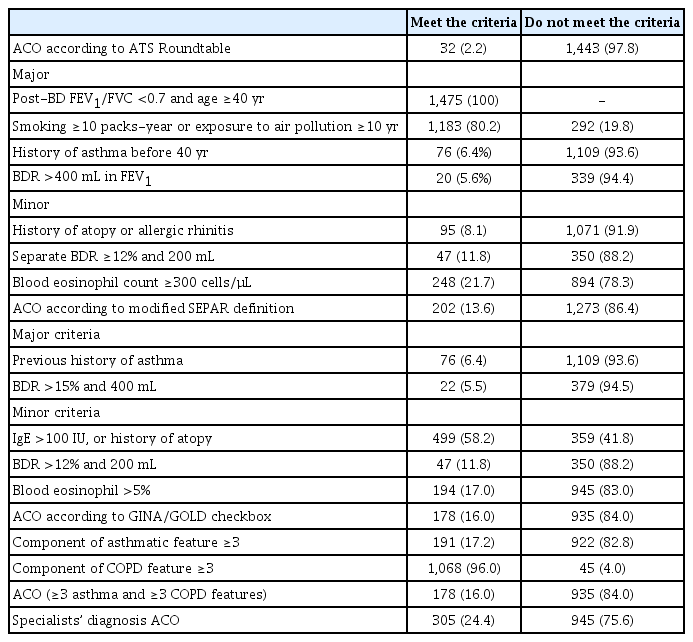
Diagnostic criteria of ACO among the study patients
2. Comparison of the clinical characteristics of the ACO and non-ACO COPD groups according to the four sets of diagnostic criteria
Baseline clinical parameters including sex, age, body mass index (BMI), smoking history, and lung function tests were compared between the ACO and non-ACO COPD groups, defined according to the four sets of diagnostic criteria (Table 2). The ACO group defined according to the ATS Roundtable criteria showed no significant difference in the proportion of males, a significantly higher number of smoking pack-years, and a higher proportion of patients with a past history of asthma and atopy (52.5 vs. 41.7, p=0.014; 65.6% vs. 4.8%, p<0.001; and 38.7% vs. 7.3%, p<0.001, respectively). The ACO group defined according to the modified SEPAR criteria showed no difference in the proportion of males, while showing a significantly lower proportion of patients with a smoking history, higher proportions of patients with a history of asthma and atopy, and a higher total IgE level and mean eosinophil count (%) (86.1% vs. 91.8%, p=0.010; 41.3% vs. 0%, p<0.001; 20.7% vs. 5.9%, p<0.001; 571.2 vs. 225.4, p<0.001; and 4.8% vs. 3.0%, p<0.001, respectively). The ACO group defined according to the GINA/GOLD criteria showed a significantly lower proportion of males, a higher BMI, and higher proportions of patients with a past history of asthma and atopy (85.4% vs. 92.7%, p=0.001; 23.7 vs. 23.1, p=0.019; 19.3% vs. 3.7%, p<0.001; and 21.4% vs. 6.3%, p<0.001, respectively). Relative to the non-ACO COPD group, the ACO group diagnosed according to specialists showed a significantly lower proportion of males, higher BMI, lower proportion of ever-smokers, higher proportion of patients with a past history of asthma and atopy, and a higher mean blood eosinophil count (%) (87.2% vs. 92.1%, p=0.009; 23.9 vs. 22.9, p<0.001; 85.4% vs. 91.6%, p=0.002; 15.4% vs. 2.8%, p<0.001; 17.1% vs. 4.9%, p<0.001; and 4.0% vs. 3.0%, p<0.001, respectively).

Comparison of clinical characteristics between the ACO and non-ACO groups according to the four different definitions
Regarding pulmonary function tests, the ACO group defined according to the ATS Roundtable criteria showed no significant difference in lung function compared to the non-ACO COPD group. The ACO group defined according to the modified SEPAR criteria showed no significant difference in FEV1 or FVC compared to the non-ACO COPD group, but had a higher residual volume to total lung capacity (RV/TLC) ratio (44.1 vs. 41.8, p=0.037). When the GINA/GOLD criteria were applied, relative to the non-ACO COPD group, the ACO group showed higher FEV1 (absolute), FEV1 (%), FVC (%), diffusing capacity of the lung for carbon monoxide (DLCO) (absolute), and DLCO (%) values (1.8 vs. 1.7, p=0.008, 71.3% vs. 64.0%, p<0.001; 90.3% vs. 86.1%, p=0.006; 14.0 vs. 13.1, p=0.021; and 78.4% vs. 73.4%, p=0.011, respectively). In terms of the COPD Assessment Test (CAT) score, the ACO group showed a higher score compared to the non-ACO COPD group (16.0 vs. 14.2, p=0.011). Relative to the non-ACO COPD group, the ACO group diagnosed according to specialists’ opinions showed higher FEV1 (%) and FVC (%) values (70.4% vs. 63.5%, p<0.001 and 89.6% vs. 85.8%, p=0.001, respectively), and a higher BDR of FEV1 (8.9% vs. 6.1%, p=0.001). They also showed better DLCO in absolute and percentage terms, and 6-minute walk distance result (14.0 vs. 12.9, p<0.001; 77.5% vs. 70.3%, p<0.001; and 422 m vs. 400 m, p=0.003, respectively).
3. Longitudinal changes in symptom scores
During the 3-year follow-up, the total St. George’s Respiratory Questionnaire (SGRQ) and CAT scores were compared between the ACO and non-ACO COPD groups defined according to the four sets of diagnostic criteria (Table 3). The ACO group defined according to the GINA/GOLD criteria showed significantly higher SGRQ and CAT scores at baseline than the non-ACO COPD group (36.1 vs. 32.0, p=0.011 and 16.0 vs. 14.2, p=0.011, respectively). However, during the 3-year follow-up, no statistically significant difference was observed between the two groups. When the modified SEPAR, ATS Roundtable and specialists’ diagnosis were applied, no statistically significant differences were found between the two groups, either at baseline or during follow-up.

Changes in symptom scores, pulmonary function, and eosinophil (%) in the ACO vs. non-ACO groups
4. Longitudinal changes in pulmonary function and eosinophil count (%)
When the GINA/GOLD criteria were applied, FEV1 (%) was significantly higher in the ACO group at baseline, and at the 1- and 2-year follow-ups, but not at the 3-year follow-up, compared to the non-ACO COPD group (71.1% vs. 64.0%, p<0.001; 67.2% vs. 61.8%, p=0.006; 67.3% vs. 61.8%, p=0.014; and 63.9% vs. 59.0%, p=0.073, respectively). FVC (%) was significantly higher in the ACO group only at baseline (90.4% vs. 86.7%; p=0.012).
The ACO group defined according to the modified SEPAR criteria showed no significant difference in FEV1 (%) or FVC (%), either at baseline or during follow-up, compared to the non-ACO COPD group. The ACO group showed a higher BDR in terms of the FEV1 (%) at the 2-year follow-up (10.0% vs. 5.8%, p=0.005). No significant group difference in FEV1 (%), FVC (%), or the BDR was seen when the ATS Roundtable criteria were applied. The ACO group defined based on specialists diagnosis showed a significantly higher FEV1 (%) than the non-ACO COPD group, at baseline and at the 1-, 2-, and 3-year follow-ups (70.6% vs. 63.4%, p<0.001; 68.2% vs. 60.7%, p<0.001; 69.4% vs. 59.9%, p<0.001; and 65.8% vs. 56.0%, p<0.001, respectively). Regarding FVC (%), the ACO group showed higher mean values, at baseline and at the 1- and 2-year follow-ups (89.9% vs. 86.3%, p=0.002; 86.1% vs. 82.3%, p=0.013; and 86.1% vs. 81.9%, p=0.026, respectively). The BDR in terms of the FEV1 (%) was also higher in the ACO group, at baseline and at the 1- and 2-year follow-ups (8.9% vs. 6.2%, p=0.001; 6.6% vs. 5.3%, p=0.048; and 8.4% vs. 5.4%, p=0.032, respectively).
When the GINA/GOLD and ATS Roundtable criteria were applied, no significant difference in blood eosinophils (%) was found between the ACO and non-ACO COPD group. The ACO group defined by the modified SEPAR criteria showed a significantly higher blood eosinophil count (%), at baseline and at the 1-, 2-, and 3-year follow-ups (4.9% vs. 3.0%, p<0.001; 4.0% vs. 3.1%, p=0.036; 4.5% vs. 2.9%, p=0.001; and 4.0% vs. 2.8%, p=0.039, respectively). The ACO group defined based on specialist diagnosis showed a higher blood eosinophil count (%) only at baseline (4.0% vs. 3.0%, p<0.001).
5. Change in lung function over 3 years
The changes in FEV1 and FVC over the 3-year follow-up were compared between the ACO and non-ACO COPD groups according to the four sets of ACO diagnostic criteria (Supplementary Table S2). The ACO group defined by the ATS Roundtable showed significantly larger decrease in percentage and absolute FVC values compared to the non-ACO COPD group (–18.9% vs. –2.2%, p=0.007; and –412 mL vs. –17 mL, p=0.036), while both the ACO and non-ACO COPD groups showed significant within-group decreases (p=0.03 and p=0.011, respectively) (Figure 1). When the modified SEPAR definition was applied, the ACO group showed a significantly larger decrease in FEV1 (%) (–4.3% vs. 0.2%, p=0.024). When the GINA/GOLD criteria were applied, the two groups did not show a significant difference in the extent of change in pulmonary function parameters over the 3-year follow-up (Figure 2). Finally, the ACO group diagnosed by specialists showed a significantly larger decrease in the FEV1 (%) compared to the non-ACO group (–5.4% vs. –0.2%, p=0.003) (Figures 1 and 2).
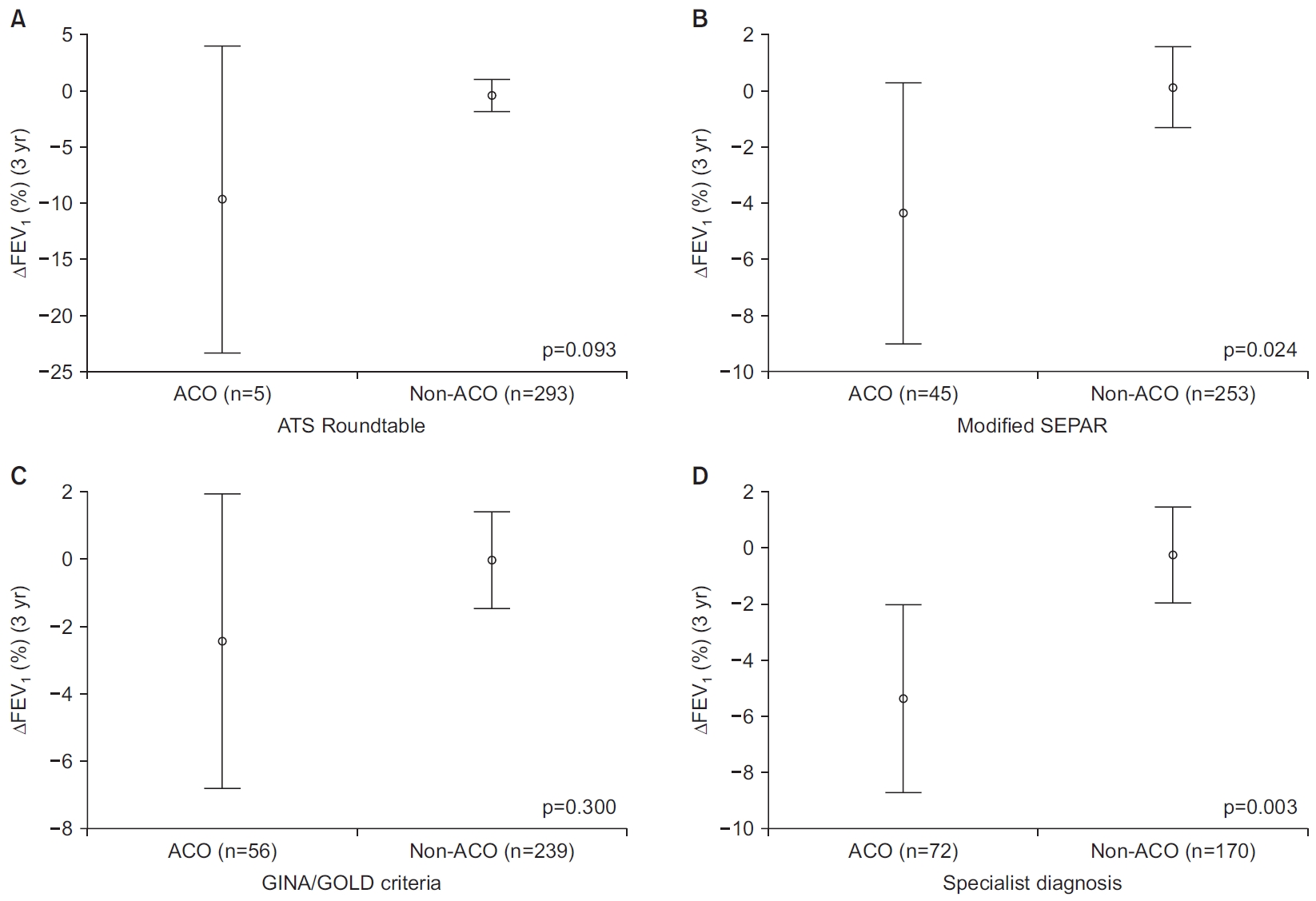
Comparison of mean values of three-year changes (with standard errors) in FEV1 (%) between the ACO group and non-ACO COPD group according to ATS Roundtable (A), modified SEPAR (B), GINA/GOLD criteria (C), and specialist diagnosis (range, 2 standard error) (D). ACO: asthma-COPD overlap; ATS: American Thoracic Society; COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 second; GINA: Global Initiative for Asthma; GOLD: Global Initiative for Chronic Obstructive Lung Disease; SEPAR: Spanish Society of Pneumonology and Thoracic Surgery.

Comparison of mean values of three-year changes (with standard errors) in FVC (%) between the ACO group and non-ACO COPD group according to ATS Roundtable (A), modified SEPAR (B), GINA/GOLD criteria (C), and specialist diagnosis (D) (range, 2 standard error). ACO: asthma-COPD overlap; ATS: American Thoracic Society; COPD: chronic obstructive pulmonary disease; FVC: forced vital capacity; GINA: Global Initiative for Asthma; GOLD: Global Initiative for Chronic Obstructive Lung Disease; SEPAR: Spanish Society of Pneumonology and Thoracic Surgery.
Discussion
This retrospective cohort study compared longitudinal changes in lung function and symptoms between ACO and non-ACO COPD groups defined according to four sets of diagnostic criteria. The results showed that the prevalence of ACO and outcomes varied according to the diagnostic criteria applied. In terms of clinical characteristics, ACO defined by specialists (based on clinical experience) and the GINA/GOLD criteria showed similar results, while ACO defined according to the ATS Roundtable criteria showed results that were inconsistent with those of the other diagnostic criteria.
Considering that the prevalence of ACO among COPD patients is 15%–30% [12-14], the prevalence of 3.3% calculated herein based on the ATS Roundtable was relatively low. This may be due to the strictness of criteria for ACO diagnosis, i.e., fulfillment of all three major criteria for ACO plus at least one minor criterion. The BDR was included among both the major and minor criteria, such that patients with no BDR (but with other asthmatic features) and patients without BDR test results are less likely to be included in the ACO group. Based on the modified SEPAR definition, 13.5% of our patients were categorized as ACO; this is similar to the study by Cosio et al. [13], in which the prevalence of ACO was 15%. Inoue et al. [15] reported that 16.6% of their patients diagnosed with COPD had syndromic features of ACO according to the GINA/GOLD criteria. Kobayashi et al. [16], using the same diagnostic criteria, reported that 14.4% of patients with COPD had ACO. These results are similar to those of our study, in which 16.0% of the patients were defined as ACO according to the GINA/GOLD criteria.
In terms of baseline clinical characteristics, the ACO groups defined according to the different criteria had clinical features similar to those of the non-ACO COPD groups. The ACO groups included lower proportions of males and ever-smokers, and showed higher BMI values and eosinophil counts (%) than the non-ACO COPD groups. The age differences between the ACO and non-ACO groups defined according to each category was not evident. This is contrary to the previous studies by Kobayashi et al. [16], and Inoue et al. [15], in which the ACO groups showed significantly younger mean age when compared to the non-ACO groups. In addition, the ACO groups had significantly higher proportions of patients with a past history of asthma and atopy, as reported in previous studies on ACO [16,17]. Compared to the other ACO criteria, the ACO group defined according to our criteria showed clinical characteristics more consistent with those reported in previous studies on ACO, including a significantly higher BDR and blood eosinophil count (%) [8,18]. The total IgE levels of the groups varied according to the diagnostic criteria applied; moreover, total IgE level was not included in all of the diagnostic criteria.
The ACO groups defined according to the modified SEPAR criteria and specialists diagnosis showed markedly larger decreases in FEV1 during the 3-year follow-up compared to the non-ACO COPD group. The ACO group defined according to the GINA/GOLD and ATS Roundtable criteria also showed a tendency toward a decline in FEV1 over the 3-year follow-up period. Lange et al. [10] reported that COPD patients with asthmatic features showed a higher rate of annual decline in FEV1, and Tkacova et al. [9] showed that ACO patients with bronchial hyperresponsiveness exhibited a faster decline in FEV1.
In all criteria, FVC decrease was more evident in the ACO groups than in the non-ACO COPD groups. We assume this change may be related to underlying diseases including cardiovascular diseases. Decreased FVC is associated with increased cardiovascular risk, especially heart failure, and underlying cardiovascular disease can also affect prognosis of COPD [19,20]. In the study by Ingebrigtsen et al. [21], the heart failure admission was more frequent in the ACO group when compare to the non-ACO COPD group. Nevertheless, underlying diseases were not evaluated in this study. This correlation is an assumption and requires a further validation in a future study.
Regarding RV/TLC, which is a parameter reported to be associated with air trapping in COPD [22], the ACO group defined according to modified SEPAR criteria showed significantly higher RV/TLC than the non-ACO COPD group in the present study. We assume that this finding may be due to the inclusion of BDR in modified SEPAR criteria. In the study by Gao et al. [23], the ACO group showed significant difference in air trapping between prebronchodialtor and postbronchodilator values, suggesting the possibility of high variability. Further studies are required for a more accurate evaluation of air trapping indexes in ACO.
The change of FVC in 3 follow-up years was large in the ACO group defined by ATS Roundtable criteria, with a mean decrease of 412 mL in 3 years. It should be taken into account that the number of patients defined as the ACO group with three-year data were too small to produce a reliable result. For a more accurate analysis, much larger number of patients are necessary. Another assumption is that air trapping has increased over 3 years in the ACO group defined by ATS Roundtable criteria. Suggested by a larger baseline value of RV/TLC in the ACO group, air trapping may have increased over 3 years and influenced FVC. However, the serial analysis of RV/TLC was not performed in our study, and a future study evaluating the interrelationship between longitudinal changes of both RV/TLC and FVC is necessary.
This study had several limitations. First, data on previous history of asthma were acquired via a questionnaire that provided relatively little information on the patient’s past medical history, which may have affected the ACO prevalence rate. Second, changes in pulmonary function were assessed only in terms of the difference between the baseline and 3-year follow-up, so the rate of decline could not be calculated. Finally, no analysis of mortality was performed.
Based on the results of this study, we believe that the ATS Roundtable diagnostic criteria for ACO may be inappropriate for clinical use in Korea due to their strictness. The GINA/GOLD and modified SEPAR criteria were similarly effective for diagnosing ACO, although the modified SEPAR criteria were superior in terms of capturing longitudinal changes in SGRQ and CAT scores. Furthermore, despite the variability among the four sets of diagnostic criteria, the ACO group always showed an overall tendency towards a more rapid decline in lung function compared to the non-ACO COPD group, such that more intensive airway management is necessary in these patients.
In the present study, prevalence and clinical characteristics of ACO varied depending on the diagnostic criteria applied. The disparities in clinical presentation and longitudinal outcomes may have resulted from different distributions of several distinct phenotypes within ACO groups, and in this context, defining ACO by specialist diagnosis may be more comprehensive and practical in clinical application.
Notes
Authors’ Contributions
Conceptualization: Lim JU, Yoon HK. Methodology: Lim JU, Yoon HK. Formal analysis: Lim JU. Data curation: Kim DK, Lee MG, Hwang YI, Shin KC, In KH, Lee SY, Rhee CK, Yoo KH. Software: Lim JU. Validation: Yoon HK. Investigation: Lim JU, Yoon HK. Writing - original draft preparation: Lim JU. Writing - review and editing: Rhee CK, Yoon HK. Approval of final manuscript: all authors.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Funding
This research was supported by grants from the Research of Korea Centers for Disease Control and Prevention (2016ER670102 and 2018ER670100), and by a grant from the Korean Academy of Tuberculosis and Respiratory Diseases (KATRD-S-2017-1).
Supplementary Material
Supplementary material can be found in the journal homepage (http://www.e-trd.org).
Criteria for diagnosis of ACO.
Change in lung function in 3 years.