



Introduction
Tobacco price increased from 2,500 KRW to 4,500 KRW in 2015 which was the sharpest hike in both relative and absolute terms contributed to a decreased smoking rate among adult men to below 40% for the first time in Korean history1. After small rebound that went over 40% in 2016, it declined to less than 40% once again and stayed at that level thereafter2. The total sales of tobacco also decreased from 4.36 billion packs in 2014 to 3.33 billion packs in 2015. However, it did not decrease further and remained at almost the same level in subsequent years. This could be attributed to the increased popularity of e-cigarettes3. It has been established that many smokers seek ways to continue smoking even in the face of increased cigarette prices either reducing other expenses to spare money for originally preferred products or switching to cheaper products4. Hence, e-cigarette could be an attractive alternative because they were exempted from the tax increase in 2015. However, economy might not be the dominant reason for the choice of e-cigarette in Korea. The gross domestic product per capita was 27,105 USD in 2015, and increased price of cigarettes, around 3.8 USD/pack would have been a negligible burden for Korean smokers. There might be more important reasons for the interest in e-cigarettes and the mental status of e-cigarette smokers might play vital role in this choice. A previous study reported that poorer mental health accounted for a higher prevalence of e-cigarette use among those with asthma5. Other studies reported that mental health problems are associated with increased risk of initiating e-cigarette among adolescents, university students, or veterans6-8. However, few studies have evaluated the mental status of ecigarette smokers among general population in Korea.
In the present study, we attempted to evaluate the prevalence of e-cigarette use, the reasons for the choice of ecigarettes, nicotine dependence, and the mental health status of e-smokers using the Korea National Health and Nutritional Examination Survey (KNHANES) data from 2013 to 2017.
Materials and Methods
1. The Korea National Health and Nutrition Examination Survey (KNHANES)
The KNHANES is a nationwide survey that has been conducted annually by the Korea Centers for Disease Control and Prevention (KCDC) to investigate the health and nutritional status of the Korean population since 1998. Since the sampling process of the KNHANES is stratified, multi-staged, and clustered based on the national census data, it assuredly represents the general Korean population9. All data were fully anonymized prior to the assessment. All procedures and terms and conditions of the survey were performed in accordance with the Declaration of Helsinki (7th version). Written informed consent was obtained from all participants prior to completing the survey. The questionnaire and dataset were provided with guidelines for calculating a health-related index indicated by the KCDC, which were available on the KCDC website (https://knhanes.cdc.go.kr/knhanes/eng/index.do). The KNHANES has been administering e-cigarette-related questionnaires since 2013, hence, this study used the KNHANES data from January 2013 to December 2017. The present study was approved by the Institutional Review Board (IRB) of Kyung Hee University College of Medicine (IRB number: KHUH 2019-10-033-004).
2. Measures
1) Smoking status
All participants were asked if they had smoked at least 100 cigarettes (5 packs) in their lifetime. If the answer was ŌĆ£no,ŌĆØ they were categorized as ŌĆ£non-smokers.ŌĆØ Those who responded ŌĆ£yesŌĆØ and who did not have experience with e-cigarettes were classified as ŌĆ£smokersŌĆØ (current- and ex-smokers all combined). Those who had experience with e-cigarettes, regardless of combustible cigarette use, were designated as ŌĆ£e-smokers.ŌĆØ We also analyzed the reasons for the use of e-cigarettes among the e-smokers.
2) Demographic data
Data on sociodemographic variables, such as age, sex, household income level, and educational level were collected. Household income and educational levels were divided into four quartiles. Comorbidities included self-reported physician diagnosis of asthma, chronic obstructive pulmonary disease, lung cancer, atopic dermatitis, and/or allergic rhinitis.
3) Nicotine dependence and the plan for smoking cessation
Based on the time between waking up and use of the first cigarette, participants were categorized into four groups: Ōēż5 minutes, 6-30 minutes, 31-60 minutes, or >60 minutes. Participants were asked if they had planned to quit smoking within a month or had stopped smoking for more than 1 day in the past year. Participants also completed a self-report questionnaire regarding smoking cessation plans, and those who planned to quit smoking within 6 months were categorized as ŌĆ£having a smoking cessation plan.ŌĆØ
4) Mental health status examination
The mental health status of participants was evaluated for perceived stress, depressive episodes, suicidal ideation/plans/attempts, and experience of consulting mental health professionals. Perceived stress was classified as ŌĆ£yesŌĆØ if the participant experienced ŌĆ£very muchŌĆØ or ŌĆ£a lotŌĆØ of stress in their everyday life. Depressive episodes were assessed using verified questionnaires. Participants were asked if they had suicidal ideation, suicide plans, or suicide attempt in the previous year.
3. Statistical analysis
Baseline characteristics were presented as percentages for categorical variables and as estimated means (┬▒standard deviation) for continuous variables. Categorical variables and continuous variables were compared using the chi-square test and StudentŌĆÖs t test, respectively. An analysis of variance using a generalized linear model with composite samples was used to determine the differences in clinical variables according to the smoking status (three groups). Multivariate logistic regression analysis and linear regression were performed after adjusting for age, sex, and smoking amount (pack-years). The analysis of mental health status according to smoking status was adjusted for income quartiles and educational levels. The results of multivariate logistic regression analyses were presented as odds ratios (ORs) and 95% confidence intervals (CIs), while those of the linear regression analysis were presented as standardized beta coefficients. A two-sided p-value <0.05 was considered significant. All statistical analyses were performed using SPSS for Windows software version 20.0 (IBM Corp., Armonk, NY, USA).
Results
1. Study population
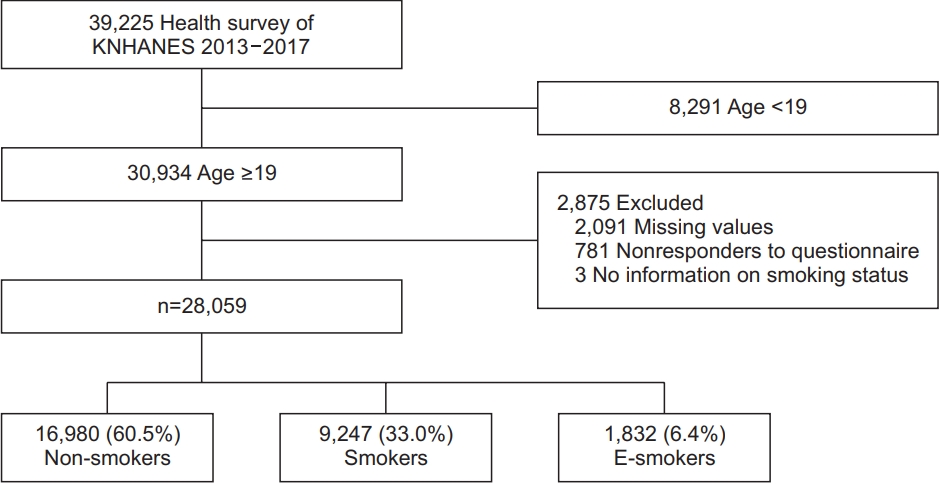
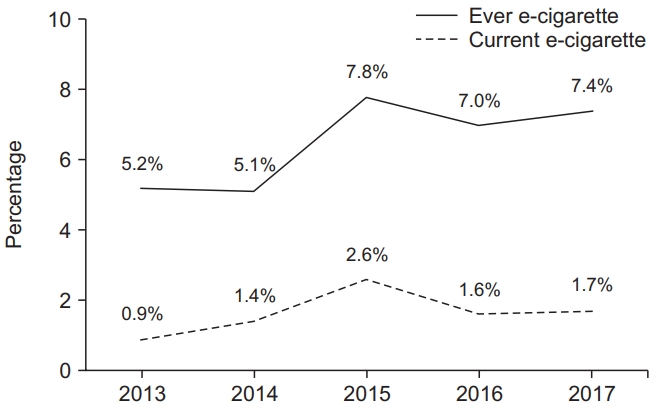
Of the 39,225 participants surveyed from 2013 to 2017, 28,059 were aged Ōēź19 years and responded to the health survey, including a questionnaire on smoking habits. Among the selected 28,059 participants, 16,980 (60.5%), 9,247 (33.0%), and 1,832 (6.4%) were non-smokers, smokers, and e-smokers, respectively (Figure 1). Most e-smokers were currently smoking combustible cigarettes (78.5%) or had previous experience with them (18.7%). The proportion of current and ever e-smokers was 0.9% and 5.2%, respectively in 2013. It peaked to 2.6% (p<0.001, p for trend=0.005) and 7.8% (p<0.001, p for trend<0.001) in 2015, when the tobacco price increased, and then stayed at that level thereafter (Figure 2).
2. Clinical characteristics
Men were more predominant in the e-smokers and smokers groups than in the non-smokers group (84.0%, 86.0%, and 16.0%, respectively; p<0.001). E-smokers were younger than smokers or non-smokers (mean ages, 39.73┬▒14.11, 53.43┬▒15.75, and 50.80┬▒17.04 years, respectively; p<0.001). The proportion of e-smokers in the upper middle and highest quartiles of household income was more than that of smokers or non-smokers (64.5%, 53.8%, and 55.8%, respectively; p<0.001). The proportion of college graduates was higher among e-smokers than among smokers or non-smokers (40.1%, 34.4%, and 33.4%, respectively; p<0.001) (Table 1).
3. Reason for choosing e-cigarettes
We analyzed the reasons for using e-cigarettes. Among 1,832 e-smokers, 840 responded to the questionnaire. The most common reason was ŌĆ£to try and quit smokingŌĆØ (46.5%), followed by ŌĆ£less harmful than combustible smokingŌĆØ (19.4%), ŌĆ£odorless than that of combustible smokingŌĆØ (16.7%), ŌĆ£good flavorŌĆØ (7.9%), ŌĆ£easy to smoke indoorsŌĆØ (3.9%), ŌĆ£tastes goodŌĆØ (0.6%), and ŌĆ£easier to obtain than combustible cigaretteŌĆØ (0.4%). Only one participant (0.1%) selected ŌĆ£the priceŌĆØ as the reason for using e-cigarettes.
4. Nicotine dependence and the plan for smoking cessation
E-smokers were more dependent on nicotine than smokers. E-smokers were more likely to smoke within 5 minutes of waking up than smokers (31.5% vs. 19.8%, p<0.001), while the latter were more likely to smoke >60 minutes after waking (36.2% vs. 19.9%, p<0.001). Regarding planned smoking cessation, the odds of having a plan to quit smoking within 6 months (OR, 1.233; 95% CI, 1.041-1.462; p=0.016) or not having smoked for more than one consecutive day in the last year (OR, 1.237; 95% CI, 1.013-1.510; p=0.037) were higher among e-smokers than among smokers (Table 2).
5. Mental health status
E-smokers were more susceptible to stress than nonsmokers or smoker. Stress was perceived as ŌĆ£very muchŌĆØ (7.0% vs. 4.4%, p<0.001) or ŌĆ£a lotŌĆØ (29.1% vs. 20.5%, p<0.001) more among e-smokers than among non-smokers. Suicidal ideation (6.5% vs. 4.7%, p<0.001), suicide plans (2.4% vs. 1.3%, p<0.001), and suicide attempts (1.1% vs. 0.5%, p<0.001) were higher among e-smokers than among non-smokers. Depressive episodes in 1 year (14.2% vs. 11.4%, p<0.05) and suicidal plans (2.4% vs. 1.8%, p<0.05) were more frequent in e-smokers than in smokers (Table 3).
Discussion
The present study investigated the prevalence of e-cigarette use, the reasons for the choice, nicotine dependence and mental health status of e-smokers using the nationally representative survey data of Korea, KNHANES (2013-2017). Ecigarettes are largely categorized into two types: closed system vaporizers (CSVs) and heated tobacco products (HTPs). The IQOS, the first type of HTP introduced in Korea was marketed on June 5, 2017, hence, almost all e-cigarettes data covered in the present study represent the CSV type of e-cigarettes.
The proportion of current and ever e-smokers in 2013 was 0.9% and 5.2%, respectively, which peaked to 2.6% and 7.8% in 2015, respectively, coinciding with the increase in tobacco prices. E-cigarettes were exempted from the tobacco tax increase in that year, making them attractive alternatives. It is natural to assume that the highest prevalence of e-cigarette smoking in 2015 was closely related to the price hike. However, contrary to our expectation, only 1 out of 840 participants (0.1%) selected price benefit as the reason for using e-cigarettes. E-smokers in the present study were more educated, and had a higher household income than non-smokers or smokers (Table 1). In other Asian countries, e-cigarette users were highly educated and economically comfortable as well10,11. This might explain why the low price of e-cigarettes was not a major reason for this choice.
The most common reason for e-cigarette use was ŌĆ£to try and quit smokingŌĆØ (46.5%), followed by ŌĆ£less harmful than combustible smokingŌĆØ (19.4%). The two, most common reasons for the use of e-cigarettes among the participants in the present study were also the most debated issues. Previous studies have shown mixed results regarding the relationship between e-cigarette use and cessation of smoking. In the United States and United Kingdom, current e-cigarette use was associated with significantly higher quitting attempts and cessation of smoking12,13. However, e-cigarette use did not promote smoking cessation or reduction of smoking among in Mexican smokers14. A more precisely designed study would be necessary to determine the relationship of e-cigarette use with quitting attempts and successful quitting in the future. The role of e-cigarette as less harmful tobacco product is also debated. The report of e-cigarette or vaping product-use associated lung injury in the United States in July 2019 raised serious concerns regarding the safety of the CSV type of e-cigarettes15. The focus concerning the relative safety of e-cigarettes has moved to the HTP type of e-cigarettes since the authorization of IQOS as a modified risk tobacco product (MRTP) by the U.S. Food and Drug Administration as of July 7, 2020. Because the present analysis mainly focused on the CSV type of ecigarettes, further discussion regarding this issue would not be continued.
Commonly, e-cigarette use (ever or current use) is more prevalent among younger age groups and men, which is consistent with our findings (Table 1)16. The demographic features of e-smokers in the present study might partly explain unstable psychology and controversial attitudes regarding nicotine dependence and the plan to quit smoking. More e-smokers smoked within 5 minutes of waking up and planned to quit smoking within 6 months than smokers (Table 2). This conflicting attitude is once again reflected in their reasons for the use of e-cigarettes. Although they wanted to quit smoking with the aid of e-cigarettes, they wanted to continue smoking because they considered e-cigarettes to be less harmful than combustible cigarettes. It is important to note that over 97% of e-smokers had experienced combustible cigarettes, and over 78% of them were current smokers of conventional tobacco. Thus, they wanted to stop smoking or at least to decrease the amount of combustible cigarette consumption, but they also wanted to continue smoking with less harmful product. This conflicting attitude of e-cigarette users explains why they are easily exploited by manufactures who claim e-cigarettes are MRTPs17. In addition, e-smokers were more susceptible to stress than non-smokers or smoker. Stress was perceived as ŌĆ£very muchŌĆØ or ŌĆ£a lotŌĆØ more among e-smokers than among non-smokers. Suicidal ideation, plans, and attempts were higher in e-smokers than in non-smokers. Depressive episodes in 1 year and suicidal plans were more frequent among e-smokers than among smokers (Table 3). The association between combustible cigarette use and subsequent depression and vice versa has been previously established18. Reportedly, dual users (those using both e-cigarettes and combustible cigarettes) tend to have a higher prevalence of depression, suicidal behaviors, or other psychiatric comorbidities than single users of each type of cigarette among adolescents19,20. The present study established that mentally unstable characteristics of e-smokers were not specifically restricted to young age group but were also applicable to the general population.
The present study had some limitations. First, the KNHANES included only adult aged Ōēź19 years. Therefore, the data of adolescents who are enthusiastic consumers of e-cigarettes were excluded in the present study. Second, we classified current and ex-smokers of e-cigarettes as e-smokers regardless the use of combustible cigarettes because pure ecigarette users accounted for only 2.8% of e-smokers. Therefore, e-smokers in the present study represent dual smokers of e-cigarettes and combustible cigarettes rather than pure consumers of e-cigarettes alone. Third, the quantity of ecigarettes consumed was not available in the KNHANES database, which made quantitative analysis impossible. Fourth, this study is an analysis of a cross-sectional study; therefore, the association in the analysis does not imply causality.
Despite these limitations, we revealed the conflicting attitudes of e-smokers with respect to nicotine dependence and their plans to quit smoking. Although, they wanted to quit smoking, they were highly dependent on nicotine. They were more susceptible to stress and had suicidal ideas and plans. All of these characteristics of e-smokers might make them easy targets for the manufacturesŌĆÖ exploitation who claim the relative safety of e-cigarette products.
In conclusion, e-smokers were younger, more educated, and had a higher income, but were more nicotine-dependent and susceptible to stress. These characteristics might make it easy for e-cigarette manufacturers to emphasize the relative safety of their products. Smoking cessation counseling should be tailored to these characteristics of e-smokers.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






