


Introduction
Giant bullae are defined as large bullae occupying at least one third of the hemithorax1. As the bullae do not take part in gas exchange and occupy space, they lead to impairment of ventilation and cause worsening dyspnea. In patients with a giant bulla, surgical bullectomy is the treatment of choice2. In 1937, Burke1 described first case of "vanishing lungs" in a 35-year-old man who experienced progressive dyspnea, respiratory failure, and radiographic and pathologic findings of giant bullae, which occupied two-thirds of both hemithoraces. Since these description, scatted reports have been described in young male smokers3. We present a case of giant bullae occupying almost the entire left hemithorax and a third of right hemithorax in young male smoker who underwent surgical bullectomy.
Case Report
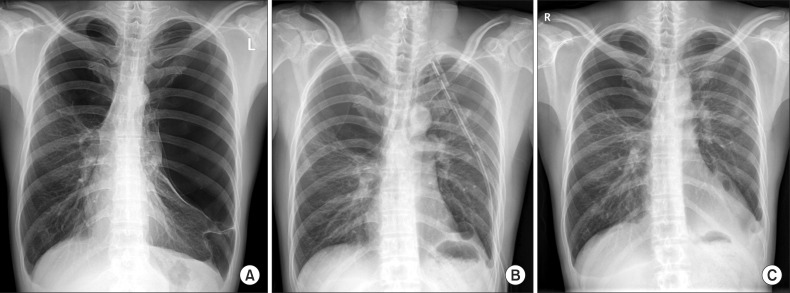
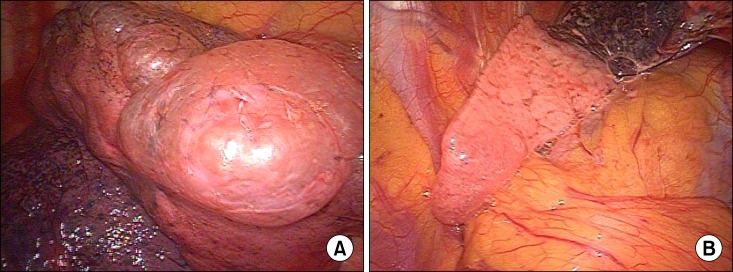
A 35-year-old man was referred to our clinic for an abnormal radiographic finding detected in screening chest X-ray. He was a current smoker with 30 pack-year and suffered from dyspnea on exertion (New York Heart Association functional class II). His chest radiography showed bilateral giant bullae occupying almost the entire left hemithorax and a third of right thorax (Figure 1A). The remaining part of the left lung was small and was compressed to the mediastinum. Pulmonary function tests revealed the following: forced vital capacity (FVC), 2.54 L (51% of predicted); forced expiratory volume in one second (FEV1), 1.57 L (40% of predicted); FEV1/FVC ratio, 0.63; diffusion capacity of the lung for carbon monoxide (DLCO), 17.4 mL/mm Hg/min (73% of predicted), and DLCO/alveolar volume (VA), 5.13 [mL/mm Hg/min]/L (114% of predicted). According to chest radiograph, giant bullae occupying nearly the entire left hemithorax with compressive atelectasis to the left lung, with the risk of impending pneumothorax. Considering limitation of his exercise capacity, elective surgical bullectomy by video-assisted thoracoscopic surgery (VATS) was performed. A left-sided, three-port technique was used to gain success to the thoracic cavity. About 28-cm-sized giant bulla originating from the apex of the left upper lobe was identified. In the surgical field, multiple bullae were detected simultaneously appeared at basal segment of the left lower lobe and the left lower lobe presented with complete atelectasis (Figure 2). Wedge resections were performed for an giant bulla at left upper lobe apex and bullae in left lower lobe basal segment using endoscopic stapling devices (Endo GIA 60). After surgical removal of bullae, one chest-tube was inserted and the collapsed left lung was re-expanded (Figure 1B). The patient was completely recovered without any event and was discharged. He remained well at the time of 1month after surgery (Figure 1C).
Discussion
Giant bullae often occur in association with emphysema. It is difficult to estimate the natural history of these bullae accurately, but their enlargement causes worsening symptoms and mechanical disturbance of ventilation4. Although spontaneous regression of a bulla is occasionally observed along with the resolution of airway pathology such as an infection, mucus plugging or tumor5, giant bulla without complications is generally characterized by gradual enlargement over time. In patients with giant bullae, bullectomy is a rather safe techinque that improves the early and late clinical and functional conditions2.
Giant bullous emphysema appears to be a distinct clinical syndrome. The disease usually afflicts young male smokers and is characterized by large bullae in the upper lobes of the lungs6. In 1937, Burke1 described first case of "vanishing lungs". Since these descriptions, scatted reports have been described in young male smokers and this entity has been referred to as the vanishing lung syndrome, type 1 bullous disease, or primary bullous disease of the lung3,7. Roberts et al.6 established the radiologic criteria for the syndromes as the presence of giant bullae in one or both upper lobes, occupying at least one third of the hemithorax and compressing surrounding normal lung parenchyma.
It's major complication is pneumothorax, which classically involves a history of acute deterioration in respiratory function associated with chest pain and also mimicking pneumothorax8. In this case, surgical bullectomy is the treatment of choice to allow the compressed lung to re-expend with a subsequent improvement of symptoms and lung function. The main factors of determine the postoperative outcome are the size of the bulla and the condition of the underlying lung. Almost normal DLCO/VA in this patients indicated that the remaining lungs seems not emphysematous and good prognostic marker for surgery.
We report a case of giant bullae, which has been removed with surgical resection. The patient was diagnosed to have a giant emphysematous bulla in the left lung on chest radiography. As far as we know, this case was the first report of giant bullae in young smoker in Korea. As shown in this report, a bullectomy via VATS could be a good option for treatment of giant bullae.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






