



Introduction
Asthma is a chronic, highly prevalent disease requiring long-term control. Although the main aim of management is to achieve and maintain good control of asthma, treatment guidelines further suggest the stepping down of therapy in patients who achieve good asthma control [1,2], which reduces both treatment cost and potential adverse effects of the medication. The Global Initiative for Asthma (GINA) recommends reducing low-dose inhaled corticosteroid (ICS) plus long-acting β2-agonist (LABA) maintenance twice daily to a once-daily regimen or completely discontinuing the LABA [1]. Many trials have confirmed that such reductions can be performed [3-5], even though the GINA recommendations are based only on clinical experience and expert opinions1. According to the recently updated GINA guidelines, as-needed low-dose ICS-formoterol is recommended in step 2 of the asthma management plan based on the evidence from recent clinical trials [6-9]. However, there is little evidence to support reducing daily low-dose ICS-formoterol maintenance to as-needed low-dose ICS-formoterol for stepping down controller treatment.
Currently, the use of a combination of low-dose budesonide (BUD) and formoterol on an as-needed regimen in mild asthma has been reported to have favorable outcomes in decreasing average annual rates of severe exacerbations [6-9]. As-needed budesonide-formoterol (BFM) is also well-tolerated and has a good safety profile [10]. Recent trials have reported that treatment with as-needed BFM is cost-effective, compared with maintenance ICS plus short-acting β2-agonist (SABA) [11,12]. However, the efficacy of this regimen during the stepping down period, particularly in patients with moderate asthma receiving low-dose BFM maintenance, has not yet been determined.
This prospective study was designed to compare the effectiveness of as-needed low-dose BFM reliever therapy with maintenance BUD plus as-needed SABA in patients with moderate asthma assessed as being in complete remission and for whom maintenance low-dose BFM therapy is recommended as step-3 of the 2020 GINA.
Materials and Methods
1. Patients
Eligible patients were adults older than 18 years, who had received a diagnosis of asthma according to the GINA 2020 criteria at least 1 year prior to study enrollment, who were assessed by the investigator and confirmed to have well-controlled asthma and were taking 3-step maintenance therapy with low-dose BFM plus SABA as needed for at least 12 weeks before randomization. The eligible patients who had complete remission were defined according to clinical remission as having well-controlled asthma based on an asthma control test (ACT) score ≥23 for at least 12 weeks [13] and Asthma Control Questionnaire 7-item version (ACQ-7) score ≤0.75 [14-16]; having fractional exhaled nitric oxide (FeNO) <25 parts per billion (ppb) [17] and blood eosinophil count (BEC) <300 cells/mm3 [18]. The exclusion criteria were current smokers or a smoking history of >10 pack-years; taking a leukotriene-receptor antagonist, xanthine derivative, and/or oral β2-agonist; previously diagnosed with a chronic pulmonary disease such as chronic obstructive pulmonary disease, chronic bronchitis, lung cancer, bronchiectasis or pulmonary fibrosis; pregnancy or planned pregnancy during the study period; history of previous lung infection, asthma exacerbation; and taking systemic corticosteroids in the past 12 weeks.
2. Study design and treatments
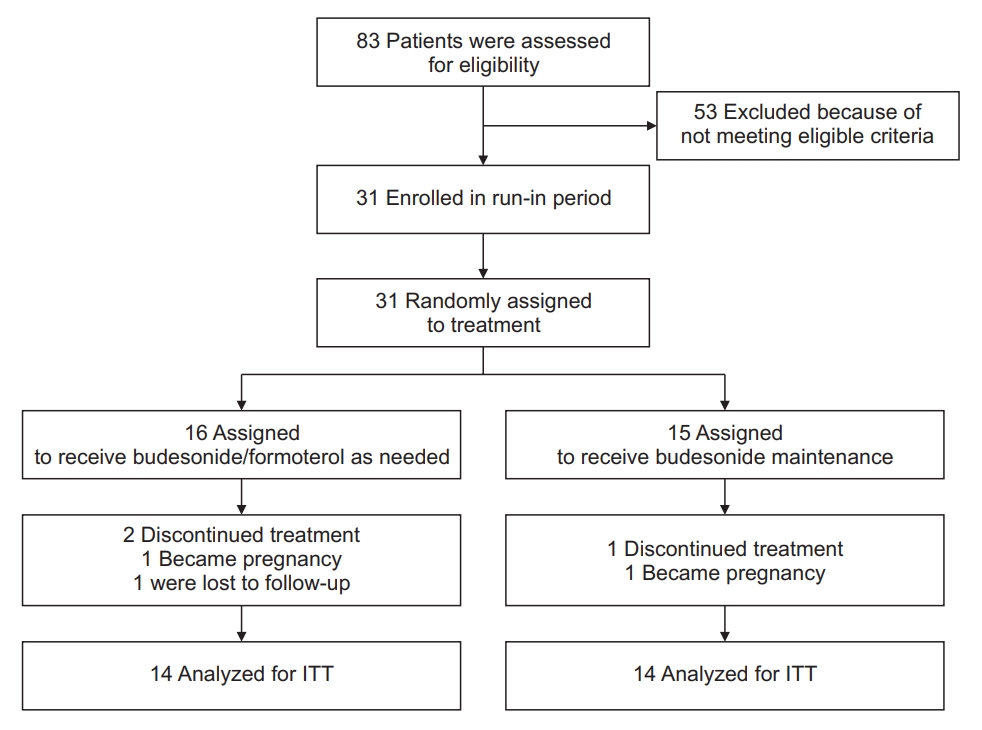
This pilot study was an open-label, randomized, parallel-group, single-center trial conducted from March 2020 to December 2021, and was registered with ClinicalTrials. gov, identifier NCT04215848. The study was done following the Good Clinical Practice guidelines and the principles of the Declaration of Helsinki, and this trial was approved by an independent Ethics committee (IRB number 15/2563). All the patients provided written informed consent prior to study enrollment. After a screening visit, patients entered a 2-week run-in period using BFM 160/4.5 µg (dry powder inhaler [DPI]; Symbicort Turbuhaler, AstraZeneca, Södertälje, Sweden), one inhalation twice daily until the day of randomization. After the run-in period, the patients were randomly assigned to a 48-week treatment period with either BFM 160/4.5 µg (DPI; Symbicort Turbuhaler, AstraZeneca) using one inhalation as needed for asthma symptoms, or BUD 200 µg (DPI; Pulmicort Turbuhaler, AstraZeneca) using one inhalation twice daily plus salbutamol from a pressured metered-dose inhaler used as needed (Figure 1). Randomization was performed using predetermined block randomization.
The patients attended the clinic for follow-up visits at 4, 8, 16, 24, 32, 40, and 48 weeks for evaluation of their asthma control status, biological markers, and pulmonary function. Asthma control status was scored using the ACT, while they were evaluated with the ACQ-7 at weeks 0, 16, 32, and 48. Spirometry, FeNO, and BEC were performed at 0, 16, 32, and 48 weeks. Baseline characteristics of all the patients including age, sex, height, body weight, body mass index, smoking history, comorbidity disease, and current medications were collected at the randomization visit. The number of BFM-as-needed and salbutamol-as-reliever inhalations were recorded on each clinic visit.
3. Outcomes
The primary outcome was the cumulative percentage of patients with treatment failure, defined as any one of the following: developing an asthma exacerbation; clinical loss of asthma control as defined by ACT score ≤20; or patient refusal to continue their study protocol because of lack of satisfaction with their asthma treatment. The secondary outcomes included the changes from baseline in the pre-dose forced expiratory volume in 1 second (FEV1) and peak expiratory flow rate (PEFR), the levels of biomarkers, BEC and FeNO, and the cumulative number of inhalations of BFM-as-needed and salbutamol-as-reliever throughout the 48-week treatment period. Adverse events were determined by non-specific questioning or direct observation by the investigator on each clinic visit and through self-reports by the patients. Asthma exacerbations were recorded as defined by the American Thoracic Society/European Respiratory Society (ATS/ERS) criteria, including a worsening of symptoms and/or lung function with increased rescue bronchodilator use lasting for 2 days or more for moderate exacerbations; the use of systemic glucocorticoid treatment for ≥3 days, or hospitalization or an emergency department visit because of asthma requiring systemic corticosteroids [19].
4. Asthma control test
The ACT instrument included four symptom/reliever questions plus a patient’s self-assessed level of control during the preceding 4 weeks with questions on limitation of activities, shortness of breath, awakenings at night, use of reliever medication, and patient’s perception of their asthma control. Each question had five response options ranging from 1-5 and a total score of 5-25; a score of 20-25 is classified as well-controlled asthma, 16-20 as not well-controlled, and 5-15 as poorly-very poorly controlled asthma [20,21].
5. Asthma control questionnaire
The ACQ is a questionnaire that measures the adequacy of asthma control and changes in asthma control status occurring either spontaneously or as a result of treatment. The ACQ has a multidimensional construct assessing symptoms (5 items self-administered) and rescue bronchodilator use (1 item-self-administered), and FEV1% (1 item) completed by the clinic staff. The questions are equally weighted and the ACQ score is the mean of the seven questions. The total score ranges from 0-6, with a score of 0.0-0.75 classified as well-controlled asthma, 0.75-1.5 as a grey zone, and >1.5 as poorly controlled asthma [16-18].
6. Spirometry
Spirometry was performed using a VIASYS spirometer (CareFusion, San Diego, CA, USA) following the standards of the ATS [22]. The highest of three values of predose FEV1, repeatable within 5%, was recorded and the predicted percent was calculated based on the reference values for healthy Thai adults. Bronchodilator reversibility was tested by having the patient inhale 400 µg salbutamol via a metered-dose inhaler after baseline testing. The percentage of reversibility was calculated based on the FEV1 or forced vital capacity changes before and after salbutamol inhalation.
8. Fractional exhaled nitric oxide
The FeNO level was measured using a portable device, NObreath (Bedfont Scientific, Maidstone, UK) which measures the level of nitric oxide in ppb in a patient’s exhalation. The patient was asked to refrain from eating nitrate-rich food, drinking caffeine or alcohol, and smoking for at least 2 hours before the test. The patient exhaled slowly with an expiratory airflow of 50 mL/sec from their total lung capacity. The mean value of two correctly performed tests was used for analysis and the FeNO level was then classified following the system of the American Thoracic Society for adults [17]. A FeNO level of less than 25 ppb indicates that the patient is receiving an adequate dosage of medication, indicating good adherence to their anti-inflammatory therapy [17].
9. Statistical analysis
The pilot study was designed to have a power of 90% and 2-sided 5% significance, resulting in a required sample size of 15 patients in each arm, and the standardized effect sizes that are medium (0.5), explained elsewhere [24,25]. Efficacy data were analyzed for an intention-to-treat population that included all the randomized patients who took at least one inhalation of the study drug and had at least one post-baseline efficacy evaluation. Missing values were accounted for using the last carried forward approach. Categorical values, expressed as numbers with proportions, were compared using Fisher’s exact test. Continuous or ordinal values were summarized as means with standard deviations or medians with interquartile ranges, and were compared by Student’s t-test or Mann-Whitney U test, respectively. The one-sample t-test was used to analyze the changes between pre- and post-stepping down treatments in the same subjects. Kaplan-Meier survival analysis, stratified by randomized treatment, was used to assess the probability of treatment failure, and the log-rank test was performed for a difference between treatments group. All the statistical analyses were performed with SPSS Statistics version 23 for Windows (IBM Corp., Armonk, NY, USA). A p-value <0.05 was considered significant, and all the tests were 2-sided.
Results
1. Baseline characteristics of the study patients
The first patient of the trial was enrolled in April 2020 and the last completed the trial in December 2021. Of the 83 patients who were screened, 53 patients (63.7%) did not meet the overall inclusion criteria and were excluded, leaving 31 patients (37.3%) to be randomized to one of the treatment groups (Figure 2). The major reason for screening failure was exceeding the cutoff level of FeNO and/or BEC. Sixteen patients were assigned to the as-needed BFM group and 15 patients to the BUD maintenance group. Three patients dropped out during treatment, leaving 28 patients to be included in the full analysis, 14 patients in each group. Table 1 presents a summary of the baseline characteristics of all the 31 patients at enrollment and randomization. There were no significant differences between the treatment groups in terms of demographic or clinical characteristics or biological markers.
2. Primary outcome
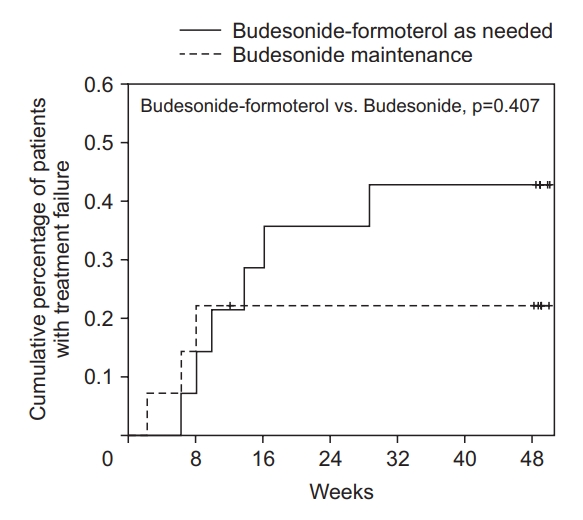
The cumulative percentages, estimated with the use of Kaplan-Meier curves, of patients with treatment failure in the two groups are shown in Figure 3. The rates of treatment failure were 42.8% and 21.4% in the as-needed BFM group and the BUD maintenance group, respectively, with an approximately 77% higher risk of treatment failure in the as-needed BFM group as compared with the BUD maintenance group (hazards ratio, 1.77; 95% confidential interval [CI], 0.44-7.12). However, there was no significant difference between the treatment group (p=0.41). Treatment failure was due to a decrease in ACT below 20 in three patients in the as-needed BFM group and one patient in the BUD maintenance group while stepping up their therapy due to patient dissatisfaction with the study drugs occurred in three patients in the as-needed BFM group and two patients in the BUD maintenance group. There were no exacerbation events in both groups during the 48-week study period.
3. Secondary outcomes
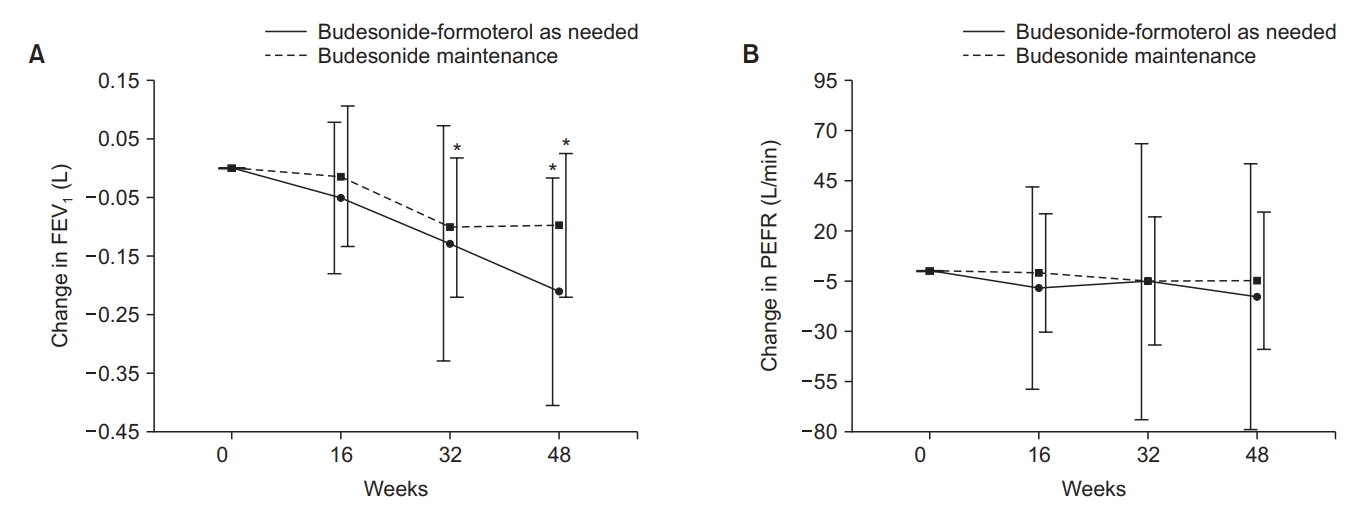
The changes in FEV1 and PEFR between baseline and each visit are shown in Figure 4. The mean absolute change from baseline in FEV1 was negatively higher with as-needed BFM than with BUD maintenance (−211.3 mL [95% CI, -373 to -48] vs. −97.8 mL [95% CI, -236 to -65]). However, this parameter did not differ significantly between treatments (p=0.75). In the as-needed BFM group, the mean FEV1 at week 48 was significantly lower than at baseline (p=0.018). In the BUD maintenance group, the mean FEV1 at weeks 32 and 48 were significantly lower than at baseline (p=0.044 and p=0.034, respectively). The mean absolute change from baseline in PEFR was also higher with as-needed BFM than with BUD maintenance (−12.9 L/min [95% CI, -42.5 to 68.3] vs. −4.9 L/min [95% CI, -21.3 to 31.2]), but the difference between the two treatments was not significant (p=0.16). In both groups, the PEFR results at each visit were modestly lower than at baseline.
For the biomarkers of airway inflammation, the mean absolute change from baseline in FeNO was higher with as-needed BFM than with BUD maintenance (8.68 ppb [95% CI, 0.46-20.64] vs. 2.5 ppb [95% CI, 0.13-20.97]), a significant difference between the treatments (p=0.047). In regards to BEC levels, there were no significant variations from baseline in either groups and the BEC levels at every visit across the study were below 300 cells/mm3 in both groups (Figure 5). The as-needed accumulative inhalations of BFM were 268 inhalations in the BFM group compared to 22 inhalations of salbutamol in the BUD maintenance group (p<0.01) (Figure 6). No adverse events were reported in either group.
Discussion
In this pilot study, we describe the effect of reducing treatment to as-needed BFM or BUD maintenance plus as-needed salbutamol in patients with moderate asthma assessed as complete remission with the use of twice-daily low-dose BFM. Our results showed different rates of treatment failure between patients taking as-needed BFM (42.8%) and those taking BUD maintenance (21.4%). However, these findings were not statistically significant. Other outcome measures, including pre-dose FEV1 and PEFR, were slightly decreased in BUD maintenance over as-needed BFM, although these differences may not be clinically important. After beginning the as-needed BFM treatment, the FeNO levels gradually but significantly increased, while remaining constant in the BUD maintenance group. The BEC levels showed only small, insignificant differences to not be affected by either treatment. In terms of the use of reliever therapy, the accumulative inhalations of BFM used as-needed were significantly higher than salbutamol used as-needed in the BUD maintenance group.
The study enrolled patients with moderate well-controlled asthma using a regular step-3 GINA maintenance treatment, although only one-third had achieved complete remission according to a previous definition explained elsewhere [26]. The majority of enrolled patients had elevated FeNO levels and/or high blood eosinophils, which was a primary concern in status of asthma control affecting the study outcomes, because either biomarkers are a significant risk factor for asthma flare-up even in patients with well-controlled asthma [27]. Therefore, all the patients had to reach the optimal levels before being enrolled in the study, this might suggest that a suppressible airway inflammation was achieved, which might have differences in responsiveness to the two treatment approaches. So, this point may affect the number of participants required for future research. Regarding lung function, although the FEV1 in the BUD maintenance group was only slightly less than the 80% predicted, we believe that the optimization and stabilization of lung function in those patients was reached. Another point to consider is that a previous study found that lung function did not correlate strongly with asthma symptoms based on validated questionnaires [28].
In this study, as-needed BFM was used in patients with well-controlled asthma who were currently on a step-3 GINA treatment prior to beginning this study on stepping down therapy, there is to date little evidence suggesting the validity of this approach. Thus, this is the first pilot study to evaluate the feasibility of using as-needed BFM as step-down controller treatment for asthma therapy. The fact that 42.8% failed the treatment with as-needed BFM, compared to 21.4% in the other group. Although the treatment failure rates may not be significantly different, these findings could indicate a trend toward a more presence of asthma symptoms and losing asthma control after using as-needed BFM. Furthermore, this finding was consistent with more accumulative inhalations of BFM in as-needed regimen, compared to those of salbutamol in the other group. One study reported that discontinuation of LABA therapy in patients with well-controlled asthma lead to deterioration of lung function and to increases asthma-associated impairment [29], however, the complete withdrawal of dual ICS and LABA therapy could have a greater effect on a worsening asthma outcomes including relapsing on airway inflammation. In the current study, the treatment with as-needed BFM resulted in significantly reduced lung function and increased levels of airway inflammation, as measured by FeNO. These findings could explain why those with as-needed BFM treatment experienced more treatment failure and a larger number of inhalations of BFM used as needed. It is known that treatment with ICS maintenance promotes the movement of FeNO toward normal levels [30,31] and withdrawal of ICS therapy results in significant increases in FeNO [32]. But comparing with SABA as needed alone, a recent study reported that as-needed BFM had more benefits in terms of suppressing airway inflammation [33]. However, the clinical significance of these FeNO differences is uncertain because the ATS guideline suggests that a change of at least 20% and 10 ppb is required to indicate a clinically significant decrease in FeNO following intervention [17]. A recent study found that neither baseline level of biomarkers nor serial measurements of FeNO are predictors for treatment failure after the stepping down of therapy to lower dosage of ICS/LABA maintenance or ICS monotherapy [34], however longitudinal studies with multiple measurements of biomarkers after reducing treatment to as-needed ICS-formoterol are needed to resolve this issue.
In recent trials, as-needed BFM was superior to maintenance ICS for reducing the risk of severe exacerbation [6,7]; however, this regimen was mainly studied in patients with uncontrolled asthma with SABA as needed or asthma controlled with ICS or leukotriene-receptor antagonist. This was not similar to our study this regimen was studied in patients with well controlled asthma having a plan to reduce the dosage of controller asthma treatment. The findings from the two studies suggest that the patients concerned about the risks or costs of daily treatment and lower doses might be helpful [35], and as-needed BFM is more cost-effective over the lifetime of patients with mild asthma[11,12]. Therefore, as-needed BFM may be an option for stepping down regardless of treatment failure. Moreover, the continuation of the same device during stepping down could be a useful strategy to overcome the problems related to poor adherence, as suggested in a previous study[36]. We found that as-needed BFM resulted in no safety problems in terms of adverse events, consistent with a recent trial, which found that BFM reliever therapy was well-tolerated in patients with mild asthma and had a safety profile similar to that of daily BUD [10].
The strengths of this pilot study are that it is the first study examining a stepping down strategy to as-needed ICS-formoterol; the 48-week duration; and the use of biomarkers to confirm suppressible airway inflammation before initiating the step-down therapy. This pilot study confirms the feasibility of the stepping down treatment and that a future full-scale research is warranted. There were some methodological limitations. First, we had a small number of participants thus leading to a considerable risk of failing to demonstrate a treatment difference; however, this is common in clinical pilot studies. Second, this was an open-label study, leading to possible performance bias. Third, although both sputum induction and bronchial provocation testing are considered reliable methods for determining airway inflammation, they were not available in our hospital so were not performed. Finally, this study did not monitor the adherence to the use of BUD, which might also have affected the study outcomes.
In summary, we found that patients whose asthma was in complete remission with the use of twice-daily low-dose BFM could be switched to a step-down treatment with as-needed BFM, however, this treatment strategy might lead to high use, as a reliever, and we did notice a trend of reduced lung function and reduction of suppressible airway inflammation. This trial demonstrates the feasibility of conducting future full-scale randomized clinical trials using uniform procedures and outcomes. However, not achieving suppressible airway inflammation as measured by FeNO and BEC in our study underscores the difficulties of enrollment to receive two treatments.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Data Sharing Statement
Data Sharing Statement Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






