



Introduction
Nontuberculous mycobacteria (NTM) are defined as a group of Mycobacterium species other than Mycobacterium tuberculosis and Mycobacterium leprae [1]. Unlike M. tuberculosis that causes tuberculosis (TB) or M. leprae that causes leprosy, NTM are opportunistic pathogens that are widespread in the environments such as soil and water [1]. An increase in the number of NTM isolation has been observed globally [2-6]. This is partly explained not only by increased awareness of symptoms caused by NTM infection and enhancements in diagnostic techniques, but also by increased numbers of susceptible hosts and the ubiquitous presence of NTM [7]. The situation is expected to become worse because most NTM either inherently possess or have the ability to acquire resistance against conventional antibiotics [8].
Currently, macrolide-based antibiotics such as clarithromycin and azithromycin are the first choice of drugs for treating most NTM infections [9]. However, treatment regimens vary by species. The regime also includes ethambutol and rifampin for slowly growing NTM [10], while it adds an aminoglycoside and either cefoxitin, imipenem, or tigecycline for rapidly growing NTM [11]. Treatment duration is prolonged up to 18 months [12]. A complete cure is not always possible [4,13]. The role of antimicrobial susceptibility testing (AST) in guiding treatment remains a subject of debate [14]. Discordance between in vitro AST and in vivo drug activity has been observed for some drugs and NTM species [12,15]. For examples, although ethambutol, rifampin, and rifabutin are clinically useful for Mycobacterium avium complex (MAC), the relationship between in vitro susceptibility results and in vivo response to antibiotics is controversial and poorly understood [16,17]. Two contradictory studies have been conducted in Korea on the relationship between in vitro AST results and treatment outcomes of ethambutol and rifampin [18,19]. AST of the second line drugs moxifloxacin and linezolid might also be taken into consideration for macrolide-resistant MAC isolates and/or isolates from patients who cannot tolerate macrolide therapy using breakpoints in Clinical and Laboratory Standards Institute (CLSI) document M62 [16]. However, the in vivo usefulness of these drugs remains unknown [20]. In addition, the evidence is limited regarding the use of in vitro AST-based treatment with injectable amikacin and beta-lactams for patients with Mycobacterium abscessus subspecies abscessus infection [21]. For Mycobacterium kansasii, there is no correlation between in vivo AST and in vivo clinical outcomes for any drugs other than rifampin [22]. These discrepancies partly originate from laboratory technical difficulties associated with AST, standardization of methods, and a lack of clinical validation [14]. Nevertheless, laboratory tests for determining AST of NTM can confirm the initial drug treatment choice and any emerging drug resistance [20]. In addition, AST may provide additional information for different drug treatment choices [20]. The prevalence of intrinsic and acquired drug resistance can also be estimated based on NTM AST in a community [20]. The goal of this study was to analyze patterns of AST for NTM isolated in a Korea tertiary university hospital and longitudinal trends of NTM identification.
Materials and Methods
1. Data collection
Mycobacterial culture and AST results were obtained from the electric medical records system from the clinical microbiology laboratory of Pusan National University Yangsan Hospital. Data were obtained for all specimens received between January 2016 and December 2020. These specimens were either from patients with presumptive mycobacterial infection or patients with confirmed TB or NTM infection. Various clinical specimens including pulmonary and extrapulmonary samples were included in this study. This study was approved by Pusan National University Yangsan Hospital Institutional Review Board (05-2021-237). Written informed consent by the patients was waived due to a retrospective nature of our study.
2. Mycobacterial culture, identification, and antimicrobial susceptibility testing
Clinical specimens were prepared according to a standard protocol [23]. Processed specimens were inoculated into BACTEC 960 mycobacterial growth indicator tubes (MGIT) (Becton Dickinson, Franklin Lakes, NJ, USA) and Ogawa media (Eiken, Tokyo, Japan) for mycobacterial culture. Liquid cultures were kept for 6 weeks. Solid cultures were examined for 8 weeks. Positive acid-fast bacilli (AFB) cultures were confirmed using Ziehl-Neelsen staining. TB/NTM differentiation was performed with an MPT 64 Ag test (SD Bioline Kit, Standard Diagnostics, Yongin, Korea) and an AdvanSure TB/NTM real-time PCR kit (LG Chem, Seoul, Korea).
Positive NTM isolates were sent to Korean Institute of Tuberculosis (KIT) for species identification and AST. NTM species identification was performed using an AdvanSure Mycobacteria GenoBlot assay (LG Chem) at KIT. The assay can identify M. tuberculosis complex and 20 different NTM species [24]. The reverse line probe assay can detect the presence of ≥2 NTM species infection in a single specimen. NTM species that could not be differentiated with the assay were confirmed by multigene sequence-based typing. Sequencing results of 16s rRNA, rpoB, and hsp65 were analyzed according to the CLSI guideline MM18-ED2 [25]. Unclassified NTM were given to NTM species that failed to be differentiated at species levels after sequencing. Discrimination between M. abscessus subspecies abscessus and M. abscessus subspecies massiliense was performed using an ERM-plus real-time PCR kit (LG Chem; commercially not available). The kit not only can differentiate between M. abscessus subspecies abscessus and M. abscessus subspecies massiliense, but also identify infection of both species in a single specimen. Mixed infection was defined as simultaneous identification of ≥2 species in a single specimen.
At KIT, AST was performed by the reference broth microdilution method for slowly and rapidly growing NTM against different drugs according to the CLSI guideline [20]. Minimum inhibitory concentration (MIC) values were analyzed using Muller-Hinton broth in polystyrene 96-well plates containing drugs in 2-fold increasing concentrations (μg/mL) (Supplementary Table S1). MIC values were categorized as susceptible (S), intermediate (I), or resistant (R) in accordance with the CLSI guideline [16] (Supplementary Table S1). To evaluate inducible resistance to clarithromycin for M. abscessus subspecies abscessus and M. abscessus subspecies massiliense, MIC values were established both at days 3 and 14 in accordance with the CLSI guideline [20]. Clinical specimens that had mixed NTM infections were also subjected to AST at KIT. However, obtaining pure culture isolates of single species was not performed prior to the broth microdilution test. We believed that this AST method for specimens was inappropriate. Hence, AST results from clinical specimens with mixed NTM infection were excluded from the current study.
3. Data analysis
The number of specimens positive for AFB culture and the proportion of NTM isolates recovered from positive specimens were calculated for each year. A linear-by-linear association exact test was used to test for significant trends. Chi-squared test and Fischer’s exacttest were used to compare differences in antimicrobial susceptibility to each drug between NTM species using SPSS for Windows version 26.0 (IBM, Armonk, NY, USA).
Results
1. Mycobacterial culture results
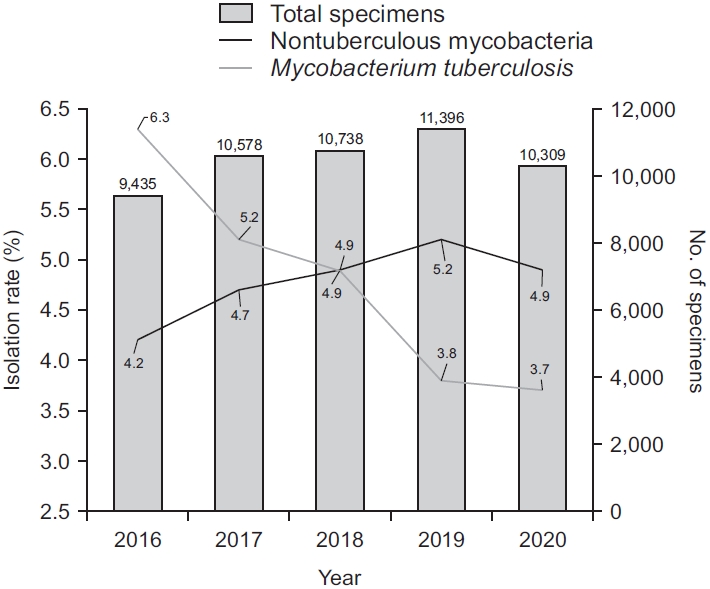
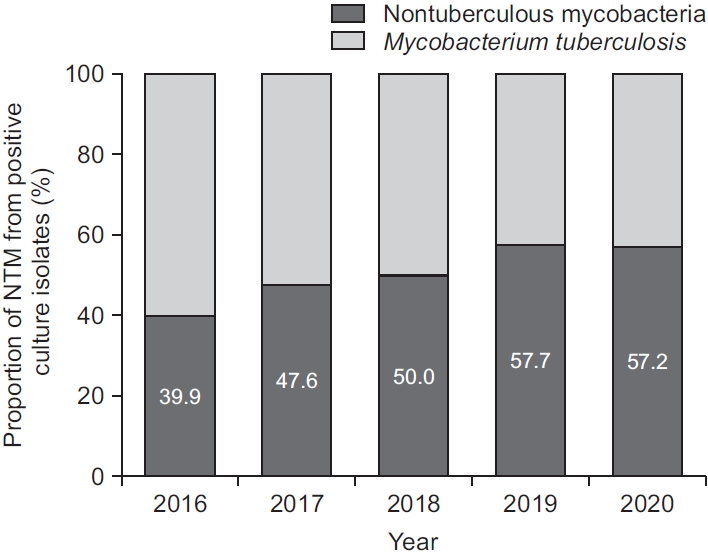
Data were obtained for 52,456 clinical specimens from 21,264 patients during the study period. The number of specimens received for mycobacterial culture steadily increased from 9,435 in 2016 to 11,396 in 2019, but decreased to 10,309 in 2020 (Figure 1). While the number of specimens positive for culture for M. tuberculosis was continuously decreased from 594 (6.3% of total specimens, 60.1% of all positive culture) in 2016 to 381 (3.7% of total specimens, 42.8% of all positive culture) in 2020, the number of NTM isolates was gradually increased from 395 (4.2% of total specimens) in 2016 to 590 (5.2% of total specimens) in 2019 (Figure 1). In total, 5,005 (9.5%) from 2,356 patients were positive for mycobacterial culture. Of these 5,005 culture positive specimens, 2,521 from 1,410 patients were positive for NTM. The proportion of NTM recovered from specimens showed an increasing trend from 39.9% in 2016 to 57.2% in 2020 (p<0.001, test for trend). Interestingly, culture positivity and proportions of NTM recovered from culture isolates were both decreased from 2019 to 2020 (Figures 1, 2).
2. Distribution of NTM species
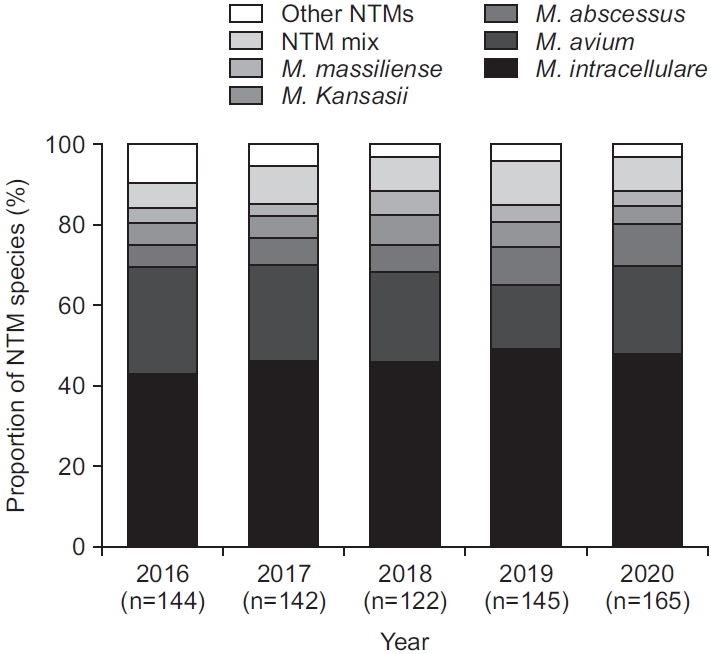
Of the 2,521 NTM cultures, species identification was obtained for 718 specimens (28.5% of 2,521) from 646 patients. Mycobacterium intracellulare (45.8%) was the most commonly isolated NTM, followed by M. avium (21.4%) and M. abscessus subspecies abscessus (7.9%) (Table 1). Interestingly, 8.5% of identified clinical isolated showed mixed NTM infection, of which a combination of M. intracellulare and M. abscessus subspecies abscessus (1.8%) was the most common, followed by mixed infection of M. intracellulare and M. avium (1.4%) (Table 1). Annual trends in distribution of NTM species recovered from clinical isolates are shown in Figure 3. The proportion of every NTM species was comparable by year (p≥0.05).
3. Antimicrobial susceptibility testing results
AST was obtained for 387 clinical specimens from 352 patients. Every isolate of M. intracellulare was susceptible to clarithromycin. Only one of 91 isolates of M. avium was resistant to clarithromycin (Table 2). It was found that 88% (191/217) of M. intracellulare isolates and 76% (69/91) (p=0.01) of M. avium isolates showed amikacin susceptibility. There was a statistically significant difference in the extent of susceptibility to moxifloxacin and linezolid between M. intracellulare and M. avium (Table 2).
For M. kansasii, 96% (22/23) of isolates showed rifampin susceptibility, while 100% (23/23) exhibited susceptibility to clarithromycin (Table 3). In general, M. kansasii showed high rates of susceptibility towards most test drugs except for ciprofloxacin and doxycycline.
Amikacin was the most effective drug against M. abscessus subspecies abscessus (92%, 35/38) and M. abscessus subspecies massiliense (100%, 18/18) (Table 4). It was found that 26% (10/38) of M. abscessus subspecies abscessus were susceptible to clarithromycin at both day 3 and day 14. At day 3, only 3% (1/38) of M. abscessus subspecies abscessus exhibited clarithromycin resistance, which was indicative of acquired resistance to the drug. It was found that 71% (27/38) of M. abscessus subspecies abscessus were susceptible or intermediate at day 3 but resistant to clarithromycin at day 14, which correlated with inducible resistance to clarithromycin. Conversely, none of M. abscessus subspecies massiliense isolates exhibited inducible resistance to clarithromycin. Instead, they all displayed the same susceptibility results at days 3 and 14.
Discussion
In accordance with past studies both from Korea and other countries [2-5], our study showed that the number of NTM isolates had increased over time. Currently, NTM constitute the majority of mycobacterial culture isolates in our hospital. Reasons behind this increase of NTM isolation are yet to be fully elucidated. Possible theories include awareness of NTM as pathogens, advancements of laboratory detection methods, increased environmental exposures, and increased numbers of susceptible patients with predisposing factors [26]. Interestingly, the number of specimens for mycobacterial culture, the number of NTM isolates, and the proportion of NTM were slightly decreased from the previous year to 2020 (Figure 1). A recent study conducted in Korea has shown that environmental exposure such as public bath is a risk factor for NTM disease [27]. The ongoing pandemic of coronavirus disease 2019 (COVID-19) has drastically changed the hygiene and sanitation procedures in public places in Korea, which might have affected patients in a way that they were less exposed to ubiquitous presence of NTM. In addition, since the number of specimens for mycobacterial culture was decreased from 2019 to 2020 (Figure 1), some patients might be less eager to seek a medical service during the pandemic. COVID-19-related social restrictions intended to control the transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) may also have been associated with decreased rates of other infectious diseases such as TB and HIV [28,29]. Our findings suggest that COVID-19 might affect recovery rates of NTM in a clinical microbiology laboratory of a tertiary hospital.
In our study, M. intracellulare and M. avium were the most common organisms recovered from clinical specimens followed by M. abscessus subspecies abscessus, consistent with previous reports from Korea [3,30]. Geographic distribution of NTM species recovered from clinical isolates can vary. For example, MAC was the most common NTM species isolated in the United States [31], whereas M. kansasii and M. abscessus complex (MABC) were the most frequent species isolated in Singapore [32] and Shanghai China [33], respectively. Such differences in the distribution of NTM species around the world can be in part due to variations in sample sources, climate changes, and population density [34]. In this study, 8.5% of all clinical specimens contained mixed infection. This proportion was similar to 7.5% in a study conducted in southwest China [35], but different from 30.1% in a study performed in Singapore [36]. Studies on isolation rates of mixed NTM infection in Korea are lacking. These results indicate that distribution of NTM multispecies infection could vary geographically as single NTM species. Although the clinical significance of mixed NTM species infection from the same patient is not fully understood yet, it is a frequent finding of NTM lung infection [35]. Disease status and clinical outcomes of patients with mixed NTM infection might be different from those with a single NTM infection [37]. Unfortunately, the correlation between mixed NTM infection and patient outcomes could not be investigated in our study due to the lack of data pertaining to clinical treatment. Misidentification of mixed NTM infection is not an uncommon finding, which can cause a critical problem in patient management [37]. Therefore, future studies should elucidate clinical outcomes of mixed NTM infection with accurate diagnosis of single or mixed NTM infection.
It has been reported that a vast majority of NTM show resistance against anti-mycobacterial drugs [38]. Although the association between in vitro AST patterns of NTM and in vivo patient outcomes was poor in previous studies [39,40], the evidence of clinical impacts of AST was observed for rifampin in M. kansasii infection [41], macrolides and amikacin in MAC infection [42,43], and macrolides in MABC [44]. CLSI’s recommendations for selecting antimicrobial agents are based on published studies about appropriate therapy [20]. Although the exact role of AST for NTM remains to be elucidated by larger clinical studies, clinical benefits of AST for NTM are manifolds [20]. First, AST results can guide treatment choices for NTM infection. Second, AST profiles might lead to better prediction of treatment outcomes. Third, detailed studies of NTM AST can be accessed by a community to estimate the prevalence of drug resistance.
MAC primary consists of M. intracellulare and M. avium. Clarithromycin and amikacin are the two first line drugs against MAC [20]. In our study, most of MAC isolates showed susceptibility to clarithromycin and amikacin, consistent with their roles in most NTM treatment regimens and correlation between in vitro susceptibility and in vivo clinical outcomes [4,42,43]. Although moxifloxacin is recommended by the CLSI as the second line drug of AST for MAC, clinical evidence is limited for clinical efficacy and safety of moxifloxacin for MAC pulmonary disease [44]. In addition, no correlation was observed between in vitro and in vivo response to moxifloxacin [45]. Clinical efficacy of linezolid, another second drug for MAC, is also uncertain [46]. According to our study, both drugs had limited activity against MAC isolates, as described in other studies [47-50].
A multidrug antibiotic regimen comprising of rifampin, ethambutol, and isoniazid is currently the recommended course of treatment for M. kansasii [46]. MIC values and clinical outcomes for ethambutol and isoniazid do not correlate well. Therefore, the current CLSI guideline does not recommend reporting in vitro AST for the drugs [16]. In addition, a short-course therapy that substitutes a macrolide for isoniazid has been proposed. However, its effectiveness has only been examined in limited studies [51]. In our study, most of M. kansasii isolates were susceptible to tested drugs except for ciprofloxacin and doxycycline, in agreement with another study [52].
MABC includes three subspecies, M. abscessus subspecies abscessus, M. abscessus subspecies bolletti, and M. abscessus subspecies massiliense [53]. Since some drugs’ susceptibility testing outcomes can only be applied to particular species, the CLSI and the majority of mycobacterial experts strongly suggest species-level identification or, in the case of the MABC, subspecies-level identification [46]. This is also required for the appropriate selection of treatment choices [46]. Our study showed that the vast majority of MABC isolates were susceptible to amikacin. For clarithromycin, we demonstrated that M. abscessus subspecies abscessus had a 71% inducible resistance rate and a 3% acquired resistance rate, which were comparable to results of a previous study [53]. However, there was a significant difference in susceptibility to clarithromycin between the two MABC species: 94% of M. abscessus subspecies massiliense were susceptible to clarithromycin, in contrast to a low susceptibility to the drug for M. abscessus subspecies abscessus (p<0.001), as observed in other studies [49,53]. The status of erm(41) gene functionality can lead to this difference in macrolide susceptibility [53,54]. These results highlight that correct identification of NTM infection is of utmost importance to guide an appropriate treatment using species-specific strategies.
Our study has several limitations. Firstly, we did not investigate the correlation of positive culture isolate with clinical or radiologic findings mainly due to the retrospective nature of this study. Given the copious number of clinical specimens, manual analysis of clinical features and radiologic findings was not possible. Thus, caution should be exercised when performing data interpretation because NTM isolation rate does not necessarily reflect the rate of NTM clinical infections. In addition, more than one spelight on the clinical significance of
cimen per patient were included in this study. Therefore, the recovery rate of NTM could be biased by this type of sampling method. Secondly, out of positive cultures for NTM, only a small portion (around 30%) were tested for species identification. In this regard, results should be interpreted with caution. Thirdly, as a tertiary hospital, most of our patients and samples came from a single province of the country. Thus, findings of this study might not be generalized to other regions or countries. In addition, the correlation between in vitro AST and in vivo clinical features was not studied, as stated previously. Future studies using patient outcomes are needed to shed light on the clinical significance of in vitro NTM AST in our hospital. Lastly, proper AST results for specimens with multispecies infection were not accomplished. Since multispecies NTM infection in a patient is not an uncommon finding, accurate AST technique using single culture isolate is necessary in the case of multispecies infection.
In summary, the recovery rate of NTM showed an increasing trend in our hospital, although the trend was not observed in 2020. It would be interesting to determine whether the COVID-19 pandemic and crisis-related regulations play a role in the change of epidemiology of NTM infection. MAC, M. abscessus subspecies abscessus, and M. kansasii were the most common NTM species in our center. Little less than 9% of total isolates were shown to be mixed NTM infection. Most of isolated NTM species were susceptible to key drugs such as clarithromycin, amikacin, and rifampin. However, most of M. abscessus subspecies abscessus isolates showed inducible resistance to clarithromycin.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Data Sharing Statement
Data Sharing Statement Full text via DOI
Full text via DOI Supplement
Supplement Print
Print Download Citation
Download Citation






