


Introduction
Advances in critical care have enabled more patients to survive from an acute catastrophic ill state; however these also created a population of patients who were dependent on continuous ventilator care and unable to recover rapidly to a point at which they were fully independent of life support1. The number of patients who require prolonged mechanical ventilation (PMV) has been increasing worldwide, and they were defined as ventilator care for ≥21 days1-10. Several studies reported that these patients consumed a disproportionately high amount of healthcare resources and medical expenses both in the intensive care unit (ICU) and after hospital discharge1-10. There were also several reports regarding prognostic factors for these patients to help physicians determine prognoses by communicating with patients or their surrogates3,11,12.
In Korea, these patients account for a significant portion of the ICU population; there would be distinct clinical characteristics and outcomes because Korea differs from Western countries in many aspects relating to medical expenses, familial support, concept of death, and social customs that would lead to distinctly different characteristics and clinical outcomes. Although there is one previous study that attempted to provide insight on this subset of patients13, it was not representative of our country's population as a whole. Thus little is known about the clinical characteristics and outcomes of patients requiring PMV in our country.
The aim of this study was to investigate the specific patterns of demographic, clinical characteristics and the objective parameter(s) related to poor prognosis in patients requiring PMV in a medical ICU of a university-affiliated tertiary care hospital.
Materials and Methods
1. Subjects
This study was conducted at Pusan National University Hospital, Busan, Korea, a university-affiliated tertiary care hospital with a 12-bed adult medical ICU with full cardiovascular and close airway monitoring, and a separate 7-bed adult coronary care unit. The physician staff in the medical ICU was comprised of 1 full-time specialist, 1 clinical fellow in pulmonary and critical care medicine, 2 resident physicians, and 1 intern. Overnight care was provided by fellow and resident physicians, while the nurse to bed ratio was 1:3. Full-time physical and respiratory rehabilitation therapies were available for all patients. Consultation services were available for all the subspecialists in the hospital.
2. Study patients
All data were derived retrospectively from the medical records of patients admitted to the adult (≥18 years old) medical ICU between January 1, 2005 and December 31, 2010. Patients with PMV were defined as those who had undergone mechanical ventilation for longer than 21 days14, regardless of the tracheostomy date. Excluded from the study were patients who had been diagnosed with irreversible brain damage, regardless of length of ICU admission. Two investigators (M.H.K. and K.L.) confirmed that the study objectives and procedures were honestly disclosed and both had full access to all data. The study protocol was approved by the Institutional Review Board (IRB) of the Pusan National University Hospital (E-2011027).
3. Data collection
The following data were gathered from the medical records of each patient: age, gender, diagnosis on initial ICU admission, Acute Physiology and Chronic Health Evaluation (APACHE) II scores on day 1 of ICU admission15, length of stay in the ICU and hospital, tracheostomy rate after admission, period from admission to the day of tracheostomy, ventilator weaning rate, ICU and hospital survival, and 6-month survival after ICU admission. The Sequential Organ Failure Assessment (SOFA) score and its components were calculated to quantify the severity of illness based on the degree of organ dysfunction16, and the simplified Therapeutic Intervention Scoring System 28 (TISS) score was calculated to assess the intensity of care on days 1 and 21 of ICU admission17. The Charlson Comorbidity Index was calculated to predict the effect of comorbid disease on patient outcome, acquired from the medical records regarding patient comorbidity before the catastrophic illness requiring ICU care18. All APACHE II, SOFA, TISS scores and Charlson Comorbidity Index were calculated from the raw data collected during chart review by the authors. Survivors were defined as patients who had survived for 6 months after ICU admission. Patients discharged without documentation of a post-discharge follow-up examination were contacted by telephone to determine the length of survival. Successful ventilator weaning was defined as breathing without assistance.
4. Statistical analysis
Statistical analyses were performed using the SPSS version 17.0 (SPSS Inc., Chicago, IL, USA). Descriptive results were expressed as mean and standard deviation or medians with range. Student's t-test was used to compare the continuous variables and the Chi-square or Fisher's exact tests (for small expected cell sizes) were used to compare categorical characteristics. Patient survival was analyzed using the Kaplan-Meier method, and compared using the log-rank test. The factors found to be significantly associated with survival were analyzed further with a Cox proportional hazard model to adjust for the potential confounding effect of each factor. Hazard ratios with 95% confidence intervals were used to report the results. A two-tailed p<0.05 was considered to indicate a significant difference.
Results
1. Clinical characteristics of patients
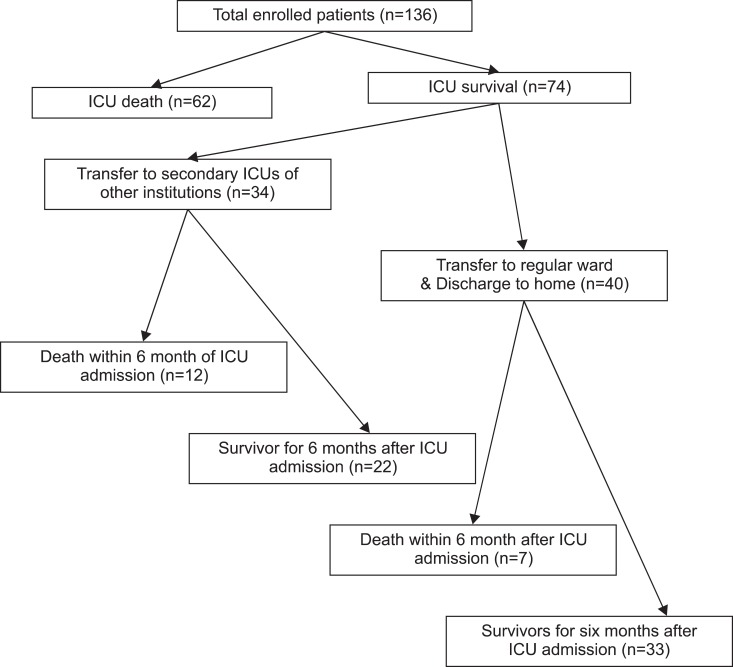
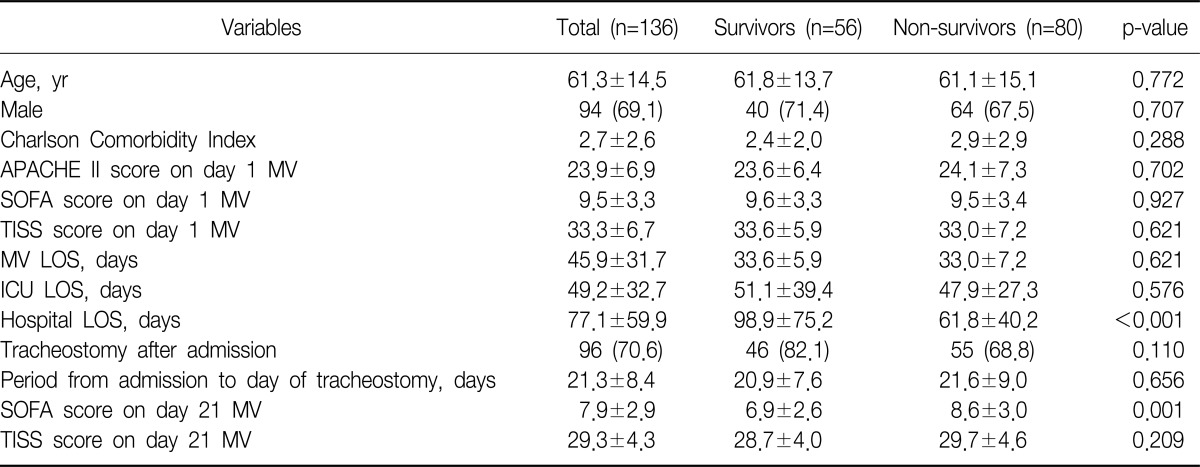
During the study period, a total of 2,644 patients were admitted to the medical ICU. Of those, 136 patients (5.1%) met our definition of PMV patients. The median number of days on mechanical ventilation was 45 (range, 21~231). Clinical characteristics of the patients are shown in Table 1. The most common diagnosis of initial ICU admission was respiratory failure caused by pulmonary causes (n=97) which included pneumonia (n=69), acute exacerbation of chronic lung disease (n=15), pulmonary tuberculosis (n=9), and pulmonary edema (n=4). The medical ICU and hospital mortality rates were 45.6% and 48.5%, respectively, and the 6-month cumulative mortality rate was 58.8%. There were 96 patients who underwent tracheostomy placement after admission and their mean period from admission to the day of tracheostomy was 21.3±8.4 days (median, 22 days; range, 1st day~50th day after admission). Among the 96 patients with trachesotomy after admission, 57 subjects (59.3%) had their placement date after 21 days of mechanical ventilation. Sixty-three patients (46.3%) were successfully weaned from ventilator care; however, we could not find any factors that were associated with successful weaning from ventilator (data not shown). Of the ICU survivors (n=74), 34 patients (45.9%) were transferred to other hospitals (not university hospitals), but there was no significant 6-month cumulative mortality difference compared to patients who were transferred to the general ward (Figure 1).
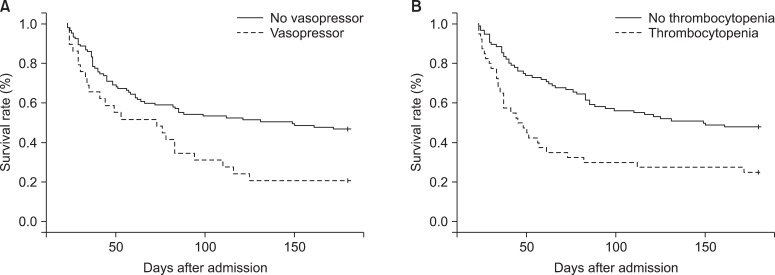
2. Predictors of survival
Aforementioned clinical factors in data collection were evaluated with regard to their influence on survival. Three factors were associated with mortality based on Kaplan-Meier survival curves and log-rank tests (p<0.05): thrombocytopenia (platelet count≤150×109/L) (p<0.001), requirement for vasopressors on day 21 (p=0.007) and tracheostomy during hospitalization (p=0.025). After adjusting for age and sex, these three factors were introduced into the Cox regression hazard model, which revealed that two variables (thrombocytopenia and requirement for vasopressors on day 21) were independent factors of survival (Table 2, Figure 2). Patients (n=57) with at least one of two factors had higher APACHE scores on admission day (25.3±7.2 vs. 22.9±6.6, p=0.044), TISS scores on day 21 (31.2±4.8 vs. 27.9±3.4, p<0.001) and 6-month cumulative mortality rates (75.4% vs.46.8%, p=0.001) than patients without these two factors.
Discussion
In this analysis of a cohort of patients with PMV, our findings were within the range compared to published studies that demonstrated the incidence of PMV patients and ventilator liberation rates in ICU2-4,6,7,13. Our study also showed a reduced 6-month cumulative mortality rate as compared to previous reports on Korean PMV patients13, which may have been due to the skilled care and advanced various medical resources of critical care. In the future, the number of patients requiring PMV is likely to increase continuously due to new therapeutic strategies and medical resources available in critical care, and would be an emerging challenge for the health care system in Korea. There is a limited amount of data about these patients in our country, thus it would be necessary to evaluate demographic and clinical characteristics through a large prospective study using a formal definition for PMV.
The definition of PMV is defined differently in other studies as ventilator care for ≥4 days with tracheostomy2,6, because the placement of a tracheostomy for patients with prolonged weaning failure is a clinical marker of the transition between the acute and chronic phases of critical illness. From the current study result, however, the period from admission to the day of tracheostomy was not constant. Also, more than half of the total number of subjects received tracheostomy after 21 days of mechanical ventilation which suggested that the day of tracheostomy and its placement may be influenced by differences of opinions between physicians and families of the patients. Therefore, it seems to be appropriate to define patients requiring PMV as those on mechanical ventilation for ≥21 days based on a consensus conference in order to obtain clear and concise clinical characteristics14.
Considering the high symptom burden of these patients and frequent poor outcomes, a mortality prediction model that identifies patients on PMV with the highest and lowest risk for death would be useful to inform discussions of prognoses among clinicians and patients or their family. Recently, a 1-year mortality prediction model was developed for these patients using clinical variables measured on day 21 including thrombocytopenia, requirement for vasopressors, hemodialysis and age ≥50 years3. Of these variables, the former two factors (thrombocytopenia and requirement for vasopressors on day 21) were prognostic indicators in the present study; however the remaining two factors (hemodialysis and age≥50 years) were not. In addition to this model, it was suggested that the long-term prognosis also would be influenced by various factors such as functional or cognitive recovery as well as the opinions of patients' family and physician-family communication6,19-21. There were also cultural differences between Western countries and Korea to be taken into consideration for providing life support; therefore it would be necessary to develop a new mortality prediction model through a multicenter study which would be applicable to the Korean patient population requiring PMV.
This study had several limitations. First, we expected that the concentration of vasopressors and degree of thrombocytopenia would affect outcomes; however, we were unable to identify any statistically significant differences, possibly due to the small sample size. Second, we could not complete interviews for survivors and survey the general conditions (such as quality of life) of the total number of enrolled patients which could have provided more significant results. Third, the study was an observational retrospective analysis and the sample size was small, in that the results of our study may not be generalized. Our data represented the experience of a single center and reflected a unique organization and process of care.
In conclusion, we found that patients requiring PMV had high 6-month cumulative mortality rates and two clinical variables measured on day 21 (thrombocytopenia and requirement for vasopressors) may be associated with prognostic indicators. Prospective, large-scale multicenter studies with longer follow-up time periods are required to determine the distinct demographic and clinical characteristics as well as prognostic factors in the Korean patient population.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






