Validity and Reliability of CAT and Dyspnea-12 in Bronchiectasis and Tuberculous Destroyed Lung
Article information
Abstract
Background
The objective of this study was to assess the validity and reliability of the Korean version of chronic obstructive pulmonary disease assessment test (CAT) and Dyspnea-12 Questionnaire for patients with bronchiectasis or tuberculous destroyed lung.
Methods
For 62 bronchiectasis patients and 37 tuberculous destroyed lung patients, 3 questionnaires including St. George's Respiratory Questionnaires (SGRQ), CAT, and Dyspnea-12 were obtained, in addition to spirometric measurements. To assess the validity of CAT and Dyspnea-12, correlation with SGRQ was evaluated. To assess the reliability of CAT and Dyspnea-12, Cronbach's α coefficient was calculated.
Results
The mean ages of the patients were 60.7±8.3 years in bronchiectasis and 64.4±9.3 years in tuberculous destroyed lung. 46.8% and 54.1% were male, respectively. The SGRQ score was correlated with the score of the Korean version of CAT (r=0.72, p<0.0001) and Dyspnea-12 (r=0.67, p<0.0001) in bronchiectasis patients. The SGRQ score was correlated with the score of CAT (r=0.86, p<0.0001) and Dyspnea-12 (r=0.80, p<0.0001) in tuberculous destroyed lung patients. The Cronbach's α coefficient for the CAT and Dyspnea-12 were 0.84 and 0.90 in bronchiectasis, and 0.88 and 0.94 in tuberculous destroyed lung, respectively.
Conclusion
We found that Korean version of CAT and Dyspnea-12 are valid and reliable in patients with tuberculous destroyed lung and bronchiectasis.
Introduction
Health-related quality of life (HRQL) is a concept which involves all aspects of physical, mental and social life. Assessment and evaluation of HRQL is very important in treating many diseases1. In chronic pulmonary diseases such as chronic obstructive pulmonary disease (COPD), asthma, and tuberculous destroyed lung, the natural course of diseases is usually progressive, and the mainstay of treatment is to improve activity and quality of daily living. Therefore, developing tools to assess these functions and quality of life is important2. In case of COPD, various tools have been developed to assess quality of life, and their validity and reliability have been well established3.
Currently, there is no disease-specific tool for assessing HRQL in tuberculous destroyed lung and bronchiectasis yet. However, St. George's respiratory questionnaire (SGRQ), which has been widely used as a tool for assessing HRQL in chronic pulmonary disease cases, has been proven to be valid and reliable by several studies4-8. However, since SGRQ is complex and time consuming to complete, it is not readily applicable in routine practice. COPD assessment test (CAT) was developed as a short, simple instrument for quantification of symptoms, and it was recently introduced after validation9,10. Modified Medical Research Council dyspnea score (MMRC) is widely used to evaluate the severity of dyspnea, but quantification of the severity using MMRC is difficult11. Dyspnea-12 is composed of 12 questions designed to assess the severity of dyspnea12. Dyspnea-12 was validated in patients with COPD10. However, validity and reliability of Korean version CAT and Korean version Dyspnea-12 questionnaire for tuberculous destroyed lung and bronchiectasis cases have not yet been confirmed. In the present study, the validity and reliability of Korean version CAT and Korean version Dyspnea-12 questionnaire are evaluated.
Materials and Methods
1. Study subjects
1) Inclusion criteria
Patients with either tuberculous destroyed lungs or bronchiectasis, who visited the outpatient clinic of Department of Pulmonology and Critical Care Medicine in Asan Medical Center and Hallym University Sacred Heart Pyeongchon Hospital between March 3, 2010 and May 3, 2011 were selected for the present study. These two institutions are university-affiliated tertiary hospitals in South Korea. Definition on each disease was made by pulmonologists as follows:
(1) Tuberculous destroyed lung; All patients with a history of treating pulmonary tuberculosis at least 1 year ago were included if more than half of one lung is destroyed on chest radiography13.
(2) Bronchiectasis; Bronchiectasis was diagnosed based on computed tomography scan findings.
2) Exclusion criteria
(1) Cases with underlying diseases considered to significantly affect the quality of life were excluded.
Heart failure
Malignant neoplasm which is not in a disease free state
History of myocardial infarction within 6 months
Severe liver diseases
Severe psychiatric diseases
Hospitalized
(2) Patients who had difficulty in filling up the questionnaire, or who did not agree to participate in the survey were excluded from the present study.
2. Methods
As a prospective cross-sectional study, informed consents in written form were collected. Then, the patients were requested to complete Korean version SGRQ, Korean version CAT questionnaire and Korean version Dyspnea-12 questionnaire by themselves. Spirometry was also performed.
1) Questionnaires
(1) Korean version SGRQ; Korean version SGRQ is composed of 50 items divided into 3 categories: symptom, activity and impact. Scores calculated from each category and the total score from all categories were analyzed and recorded, respectively. Scores range from 0 to 100 where 0 is the best HRQL, and 100 the worst4. In the present study, Korean version SGRQ was used, which was previously validated5.
(2) Korean version CAT questionnaire; Korean version CAT questionnaire is composed of 8 items. Each item has a score ranging from 0 to 5, thereby making the total score range from 0 to 40. Score of 0 represents the best quality of life and 40 does the worst9. Korean version CAT questionnaire was used after obtaining permission from GSK (GlaxoSmithKline).
(3) Korean version Dyspnea-12 questionnaire; Korean version Dyspnea-12 questionnaire is composed of 12 items requiring either one of the 4 types of responses: none, mild, moderate or severe. Each response receives scores ranging from 0 to 312. The original version of Dyspnea-12 questionnaire was first translated into Korean under permission of the original author of the questionnaire. The quality of translation was again confirmed by the original author after translation and thorough revision.
2) Spirometry tests
Using a spirometer (Vmax22 or 2130; Sensor Medics, Yorba Linda, CA, USA), forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) were measured. Spirometry was conducted following the method recommended by American Thoracic Society and European Respiratory Society. With respect to normal predictive values of spirometry, the Korean reference equation reported by Choi et al.14 was used.
3) Statistical analysis
In order to evaluate validity, correlation analysis was conducted using Pearson's correlation. The association between the scores of Korean version CAT questionnaire and the scores of the Korean version SGRQ, and that between the score of Korean version CAT questionnaire and the FEV1 were evaluated. Similarly, for the scores of Korean version Dyspnea-12 questionnaire correlation analysis was underwent to evaluate its association with Korean version SGRQ and FEV1. To assess reliability, Cronbach's α coefficient was calculated determining the internal consistency of Korean version CAT questionnaire and Korean version Dyspnea-12 questionnaire. Using SAS for Window version 18.0 (SPSS Inc., Chicago, IL, USA), statistical analysis was conducted. All data are expressed means and standard deviations or frequencies. Statistical significance was accepted for p-values less than 0.05.
4) Approval from Institutional Review Board (IRB)
Approval from IRB of Asan Medical Center and Hallym University Sacred Heart Pyeongchon Hospital was obtained. Written informed consents from all participants were collected.
Results
1. Bronchiectasis
1) Patient characteristics
Sixty two patients were enrolled to this study and their mean age was 60.7 years. Most of patients in study cohort were female and non-smokers (Table 1). In average, spirometry showed mild airflow obstruction.
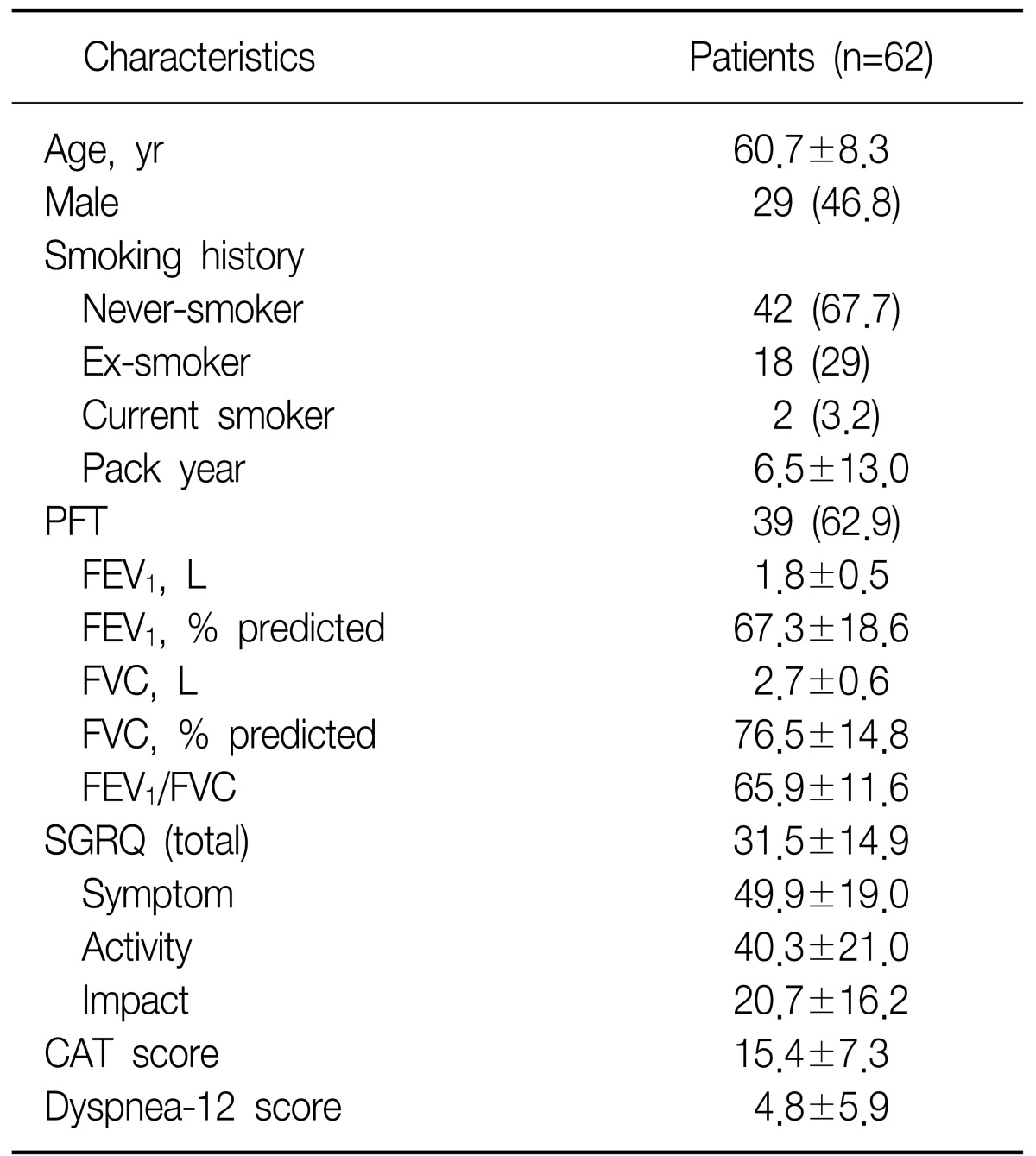
Characteristics of bronchiectasis patients
2) Correlation between Korean version CAT questionnaire or Korean version Dyspnea-12 questionnaire, and Korean version SGRQ
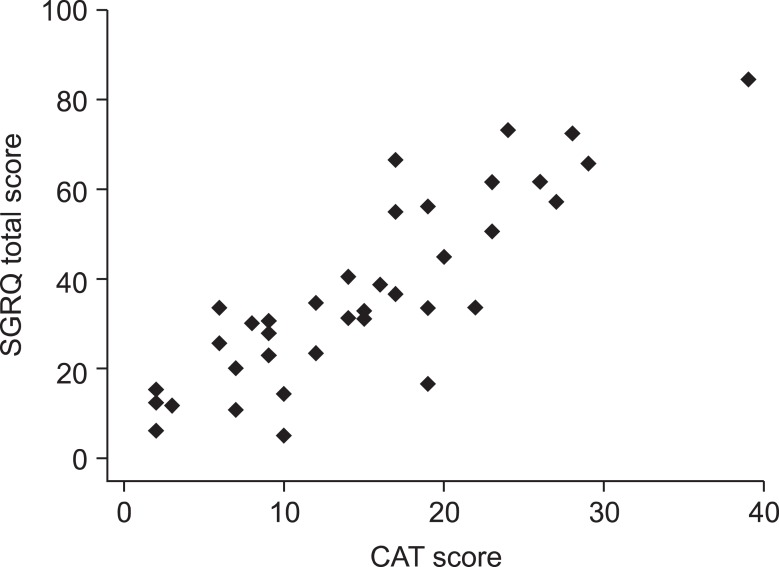
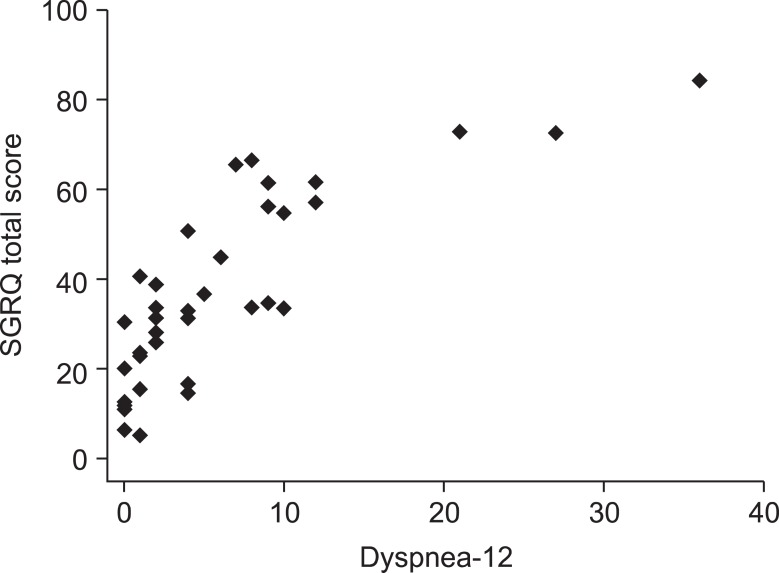
The Korean version CAT questionnaire was strongly correlated with the Korean version SGRQ (Figure 1). Korean version Dyspnea-12 questionnaire also showed a significant correlation with Korean version SGRQ (Figure 2).

Correlation between chronic obstructive pulmonary disease assessment test (CAT) score and St. George's Respiratory Questionnaire (SGRQ) total score in bronchiectasis patients (r=0.72, p<0.0001; 62 patients).

Correlation between Dyspnea-12 score and St. George's Respiratory Questionnaire (SGRQ) total score in bronchiectasis patients (r=0.67, p<0.0001; 62 patients).
3) Distribution and internal consistency of Korean version CAT questionnaire and Korean version Dyspnea-12 questionnaire
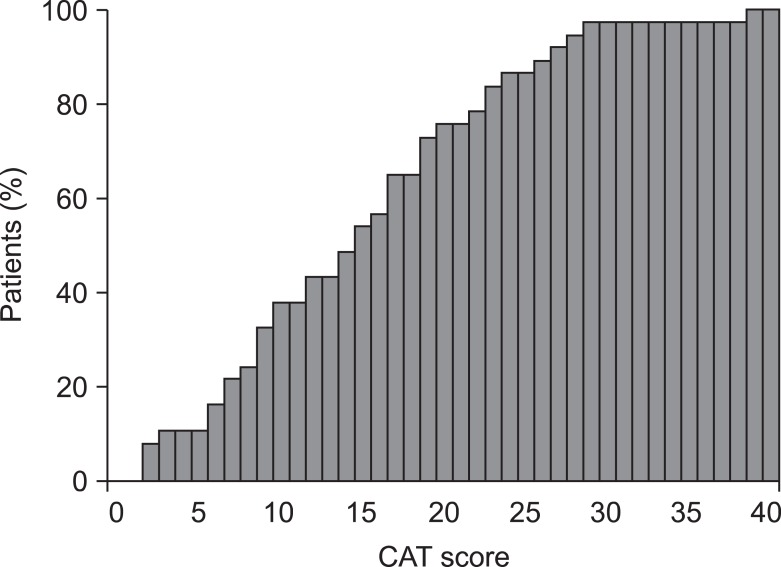
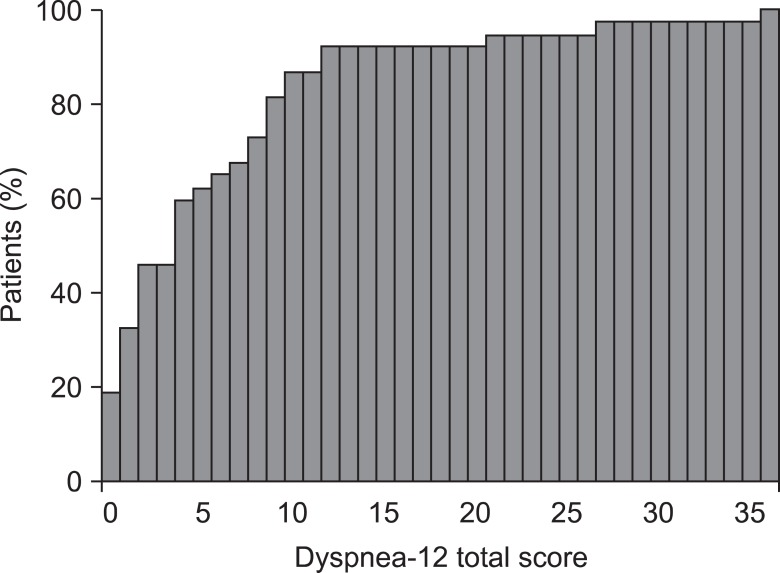
Most subjects scored 10 and 14 in Korean version CAT questionnaire (n=5, 8.1%), and total score was below 20 in 75% of the subjects (Figure 3). Most of the subjects scored 0 in Korean version Dyspnea-12 questionnaire (n=15, 24.2%), and 36 (51.6%) of the subjects scored from 0 to 3, implying that the scores of Korean version CAT questionnaire and Korean version Dyspnea-12 questionnaire were distributed mainly in the low-score range (Figure 4). Cronbach's α coefficients representing internal consistency of Korean version CAT questionnaire and Korean version Dyspnea-12 questionnaire were 0.84 and 0.90, respectively.
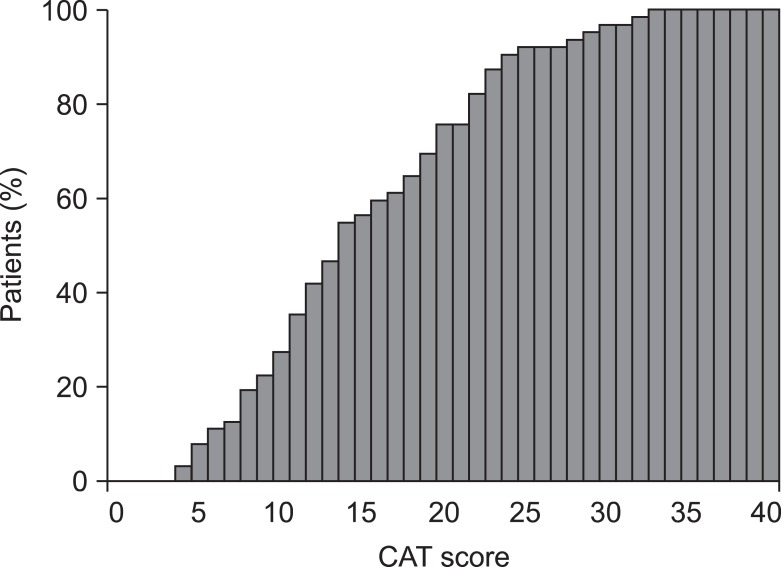
Cumulative frequency distribution of chronic obstructive pulmonary disease assessment test (CAT) score in 62 bronchiectasis patients.
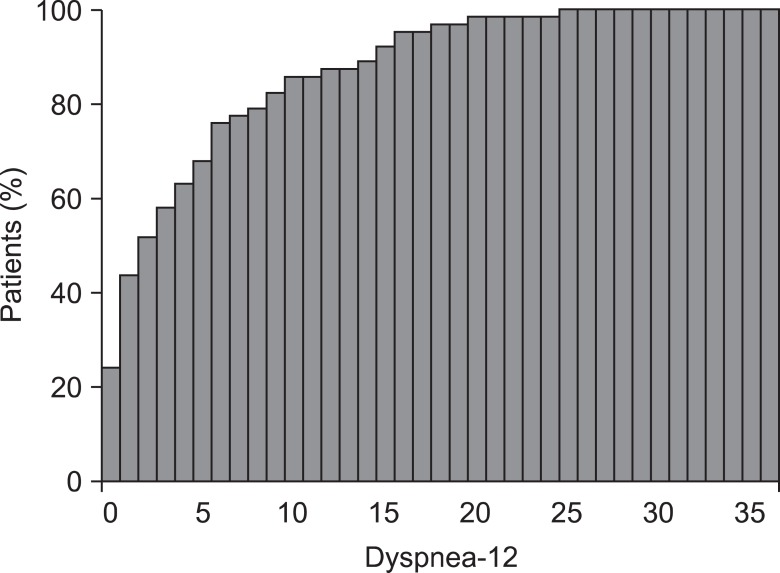
Cumulative frequency distribution of Dyspnea-12 score in 62 bronchiectasis patients.
4) Correlation between Korean version CAT questionnaire or Korean version Dyspnea-12 questionnaire, and pulmonary function test
In patients with bronchiectasis, no significant correlation was observed between Korean version CAT questionnaire and pulmonary function test. With Korean version Dyspnea-12 questionnaire, both FEV1 and FVC showed a significant negative correlation (Table 2).

Correlation between the questionnaires and pulmonary function test in 62 bronchiectasis patients
2. Tuberculous destroyed lung
1) Characteristics of the subjects
Thirty seven patients were enrolled to this study and their mean age was 64.4 years. Most of the subjects were male and non-smokers (Table 3).
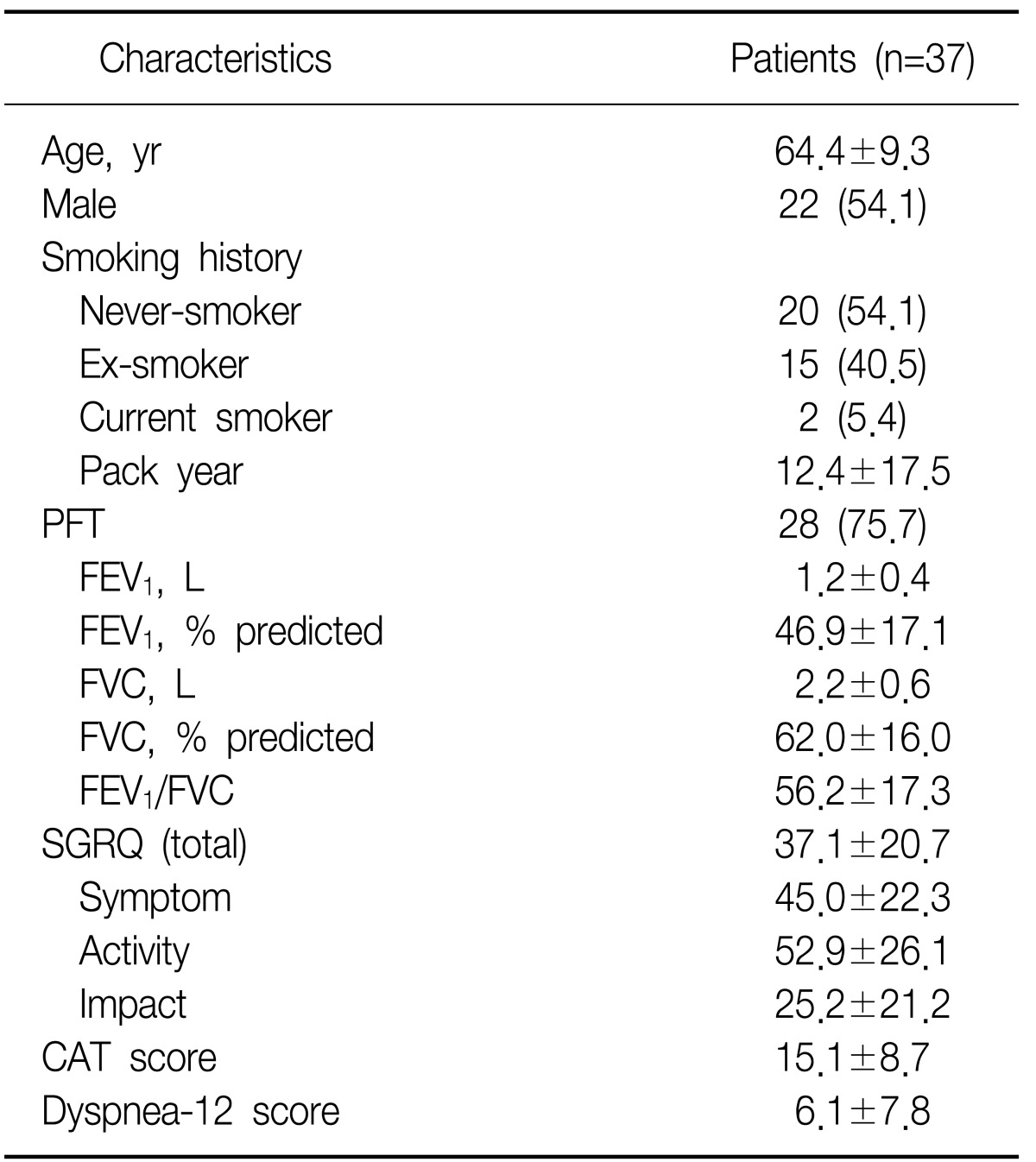
Characteristics of tuberculous destroyed lung patients
In average, spirometry showed moderate airflow obstruction.
2) Correlation between Korean version CAT questionnaire or Korean version Dyspnea-12 questionnaire, and Korean version SGRQ
The Korean version CAT questionnaire was strongly correlated with the Korean version SGRQ in patients with tuberculous destroyed lung (Figure 5). In addition, Korean version Dyspnea-12 questionnaire also showed a significant correlation with Korean version SGRQ (Figure 6).
Correlation between chronic obstructive pulmonary disease assessment test (CAT) score and St. George's Respiratory Questionnaire (SGRQ) total score in tuberculous destroyed lung patients (r=0.86, p<0.0001; 37 patients).
Correlation between Dyspnea-12 score and St. George's Respiratory Questionnaire (SGRQ) total score in tuberculous destroyed lung patients (r=0.80, p<0.0001; 37 patients).
3) Distribution and internal consistency of Korean version CAT questionnaire and Korean version Dyspnea-12 questionnaire
According to the result of Korean version CAT questionnaire, a 73% of the subjects scored less than 20 (Figure 7). In Korean version Dyspnea-12 questionnaire, most of the subjects scored 0 (n=7, 18.9%), and 22 (45.9%) of the subjects scored from 0 to 2, implying that the scores of Korean version CAT and Korean version Dyspnea-12 questionnaire were distributed mainly in the low-score range (Figure 8). Cronbach's α coefficients representing internal consistency of Korean version CAT questionnaire and Korean version Dyspnea-12 questionnaire were 0.88 and 0.94, respectively.
Cumulative frequency distribution of chronic obstructive pulmonary disease assessment test (CAT) score in 37 tuberculous destroyed lung patients.
Cumulative frequency distribution of dyspnea-12 score in 37 tuberculous destroyed lung patients.
4) Correlation between Korean version CAT questionnaire or Korean version Dyspnea-12 questionnaire, and pulmonary function test
No significant correlation was observed between Korean version CAT questionnaire and pulmonary function test in patients with tuberculous destroyed lung. Korean version Dyspnea-12 questionnaire did not show a significant correlation with pulmonary function test, either (Table 4).

Correlation between questionnaires and pulmonary function test in 37 tuberculous destroyed lung patients
Discussion
The results from this study demonstrated that the Korean version CAT questionnaire and the Korean version Dyspnea-12 questionnaire are significantly correlated with the Korean version SGRQ in patients with bronchiectasis and also those with tuberculous destroyed lung. Also, its internal consistency appeared to be good. We used Pearson's correlation analysis for convergent validity and Cronbach's α coefficient was applied to confirm internal reliability.
The annual incidence of pulmonary tuberculosis is still globally high with approximately 8.8 million15. Although patients can be microbiologically cured with appropriate treatment, it can result in residual anatomical and functional changes16. Moreover, the burden of diseases affecting HRQL is considered to be high, but only a few studies have been conducted regarding the HRQL of patients with tuberculous destroyed lung.
Bronchiectasis is a disease characterized by the irreversible bronchial dilation and deformity as a result of the destruction of bronchial muscle and its elastic tissue. Symptoms include cough, sputum and dyspnea, which are similar to those of COPD and tuberculous destroyed lung17. In present study, we evaluated the validity and reliability of Korean version CAT questionnaire, which was previously developed as a simple tool for assessing quality of life in patients with COPD, in patients with bronchiectasis and tuberculous destroyed lung. To our knowledge, there has not been a disease-specific tool to assess HRQL in these diseases, to date.
In our study, the correlation between the results of pulmonary function test and the scores of Korean version CAT questionnaire was found to be low and statistically insignificant. In previous studies, significant, but low correlation between pulmonary function test results and SGRQ in chronic pulmonary disease have been reported5-7. Similar result was reported by another study regarding the validity and reliability of Korean version CAT in COPD patients10. These results reflect that each individual's physiological profile such as FEV1 does not necessarily determine one's quality of life by itself. However, the significance of these correlation analyses might have been underestimated due to small sample size.
The study results showed that both Korean version CAT score and Korean version Dyspnea-12 Questionnaire score were distributed at a relatively low-score range. This type of distribution might be due to the fact that most patients participated in this study visited outpatient clinics with moderate to mild symptoms. However, despite this limitation, these assessment tools may be applicable to patients in routine practice as most patients in routine practice are clinically stable.
Korean version CAT questionnaire does not have any item to assess hemoptysis and recurrent infection which are common symptoms of bronchiectasis, and accordingly, this might have limited reflecting disease-specific aspects. Since this was not evaluated in our study, further studies will be required to determine whether Korean version CAT questionnaire reflects the changes in disease-specific symptoms or symptoms accompanied by exacerbation.
In summary, we have confirmed the validity and the reliability of Korean version CAT questionnaire and Korean version Dyspnea-12 questionnaire in patients with bronchiectasis and tuberculous destroyed lung. Since these two questionnaires are composed of simple items, patients can easily complete in a short period of time, thereby making them more convenient tools for assessing quality of life in routine practice.
Acknowledgements
This study was supported by a grant of the Korea Healthcare Techonology R&D project, Ministry for Health and Welfare, Republic of Korea (A102065).