Impaired Expression of MAPK Is Associated with the Downregulation of TNF-α, IL-6, and IL-10 in Mycobacterium abscessus Lung Disease
Article information
Abstract
Background
Healthy individuals who develop nontuberculous mycobacteria (NTM) lung disease are likely to have specific susceptibility factors which can lead to a NTM infection. The aim of the present study was to investigate the mechanism underlying innate immune responses, including the role of mitogen-activated protein kinase (MAPK), in Mycobacterium abscessus lung disease.
Methods
Extracellular signal-regulated kinase (ERK1/2) and p38 MAPK expression in monocytes from peripheral blood mononuclear cells were measured by Western blot analysis after stimulation by Mycobacterium avium in five patients with M. abscessus lung disease and seven healthy controls. A M. avium-induced cytokine assay was performed after inhibition of ERK1/2 and p38 MAPK pathways.
Results
Mycobacterium avium induced p38 and ERK1/2 expression in monocytes from healthy controls and subsequently upregulated tumor necrosis factor (TNF)-α, interleukin (IL)-6, and IL-10 production. In monocytes from patients with M. abscessus lung disease, however, induction of p38 and ERK1/2 expression, and the production of TNF-α, IL-6, and IL-10 were significantly lower.
Conclusion
Decreased activity of MAPK and cytokine secretion in monocytes from patients with M. abscessus lung disease may provide an explanation regarding host susceptibility to these uncommon infections.
Introduction
Mycobacterium abscessus belongs to a group of rapidly growing mycobacteria that cause a wide spectrum of infections in humans including pulmonary, skin, soft tissue, and bone disease1,2. Since M. abscessus is resistant in vitro to many antibiotics, obtaining a successful treatment outcome is difficult, especially in patients with pulmonary disease3-6.
Numerous lung diseases cases associated with nontuberculous mycobacteria (NTM), including M. abscessus, are elderly women without predisposing risk factors such as preexisting lung disease or demonstrable immunodeficiency2,7-10. Since NTM are ubiquitous in the environment (e.g., soil and water) and disease occurrence is uncommon, normal host defense mechanisms must be sufficiently effective to prevent infection8. Therefore, otherwise healthy individuals who develop NTM lung disease are likely to have specific susceptibility factors that lead to NTM infection.
Toll-like receptors (TLRs) play a critical role in the recognition of mycobacterial infection and function in the host's innate defense response11-13. TLR2 is reportedly required for NTM signaling and increased rates of M. avium infection are observed in TLR2-knockout mice14. Mitogen-activated protein kinases (MAPKs), which are triggered by mycobacteria through engagement of TLRs, are important signal-transducing enzymes involved in many facets of cellular regulation and cytokine responses15,16. The MAPK family is composed of three major serine-threonine protein kinases including p38, extracellular signal-regulated kinase (ERK1/2), and the c-Jun NH2-terminal kinase15.
Several studies have been performed on MAPK signaling in macrophages during NTM infection17-19, which suggested that the degree and timing of p38 and ERK1/2 activation contribute differently in response to mycobacterial organisms. While ERK1/2 or p38 signaling are responsible for the induction of tumor necrosis factor (TNF)-α, a key cytokine involved in granuloma formation during NTM infection, p38 is primarily involved in the initiation of interleukin (IL)-10, which is an anti-inflammatory cytokine18,20. MAPK p38 and IL-10 pathways might be associated with the survival of mycobacterium in the macrophages18,19,21,22. Studies on NTM stimulated MAPK pathway have been performed in human cells12,20, but few studies have examined the MAPK pathway in human patients with NTM lung disease as compared to healthy controls.
Our previous study suggested that the downregulation of TLR2 and the resulting decreased production of IL-12 p40 and TNF-α following stimulation of M. avium may contribute to host susceptibility to NTM lung disease11. MAPKs engage TLRs when they initiate the immune response15,16. Therefore, we assessed whether the expression of MAPKs, known as a critical enzyme in immune responses during NTM infection, contribute to susceptibility in patients with M. abscessus lung disease as compared to healthy controls.
Materials and Methods
1. Study population
The present study included five patients with M. abscessus lung disease and seven healthy volunteers. The diagnosis of M. abscessus lung disease was made according to the diagnostic criteria published by the American Thoracic Society2. All patients had characteristic findings on high-resolution computed tomography scans, such as bilateral bronchiectasis combined with multiple small nodules and branching linear structures23. Baseline characteristics of patients are presented in Table 1. M. abscessus was identified using a polymerase chain reaction and restriction length polymorphism method based on the rpoB gene, as previously described24. Peripheral blood samples of 30 mL were obtained from the controls and patients before antibiotic therapy was initiated. This study was approved by the Institutional Review Board at our institution and written informed consent was obtained from all participants.
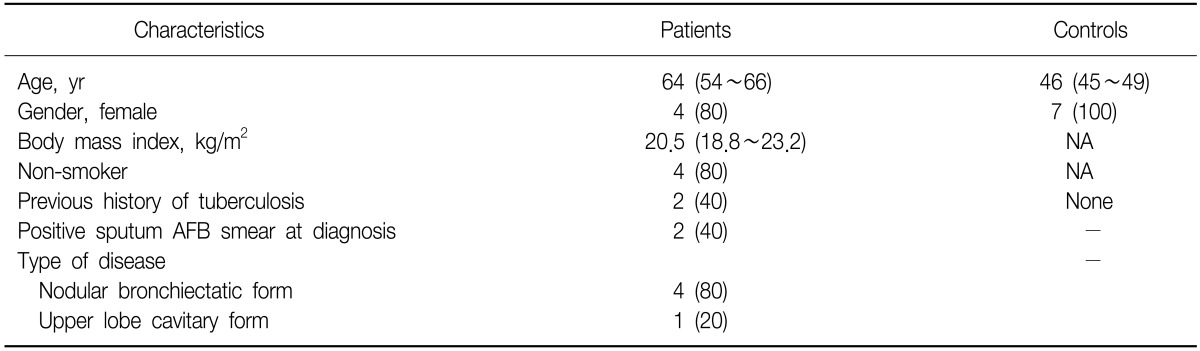
Baseline characteristics of five patients with Mycobacterium abscessus lung disease and 7 healthy controls
2. Preparation and stimulation of human monocytes
Peripheral blood mononuclear cells (PBMCs) were separated from heparinized whole blood using standard density gradient centrifugation with Ficoll-Paque™ (GE-Healthcare, Uppsala, Sweden). Cells were incubated for 1 hour at 37℃, and non-adherent cells were removed by pipetting off the supernatant. Adherent monocytes were then resuspended at a density of 1×105 cells/well in RPMI-1640 medium (Life Technologies, Grand Island, NY, USA) for the cytokine assay and at a density of 3×105 cells/well for the MAPK assay.
Monocytes were stimulated with either M. avium (American Type Culture Collection 25291; ATCC, Manassas, VA, USA) which was obtained from the Korean Institute of Tuberculosis, at a multiplicity of infection (MOI) of 70 or lipoteichoic acid (LTA) from Staphylococcus aureus (10µg/mL; InvivoGen, San Diego, CA, USA) and incubated at 37℃ for 18 hours. The preliminary data of healthy human sample under different MOI showed peak level of TNF-α production over MOI of 50. Cell-free (cleared) supernatant fractions were collected and analyzed for cytokine release.
3. Cytokine assay
Culture supernatants were collected at 18 hours to examine cytokine release from monocytes following M. avium and LTA stimulation. The concentrations of IL-10, IL-6, and TNF-α in the culture supernatants were measured using commercially available enzyme-linked immunosorbent assays kits (BioSource, Camarillo, CA, USA).
Cytokine concentrations in samples were calculated using standard curves generated from recombinant cytokines, and the results were expressed in picograms per milliliter.
4. Signaling inhibition assays
Human monocytes (3×105 cells/well) were pretreated with 10µg/mL of anti-TLR2-specific antibody (eBioscience, San Diego, CA, USA), 10µg/mL of the p38 signaling inhibitor SB203580 (Calbiochem, San Diego, CA, USA) or 20µg/mL of the ERK1/2 selective inhibitor PD98059 (Calbiochem) for 90 minutes prior to stimulation. Cells were then stimulated with M. avium or LTA. Culture supernatants were harvested and assayed for cytokine activity.
5. p38 and ERK1/2 assays
Following stimulation, the human monocytes (3×105 cells/well) were harvested and lysed. For Western blot analysis, samples were separated on 8% sodium dodecyl sulfate-polyacrylamide gel electrophoresis, transferred to a polyvinylidene difluoride membrane (Invitrogen Life Technologies, San Diego, CA, USA), and immunoblotted with the antibodies anti-phospho-p38, anti-p38, anti-phospho-ERK, anti-ERK (Cell Signaling Technology, Danvers, MA, USA), and anti-β-actin (Santa Cruz Biotechnology, Santa Cruz, CA, USA). The reaction was detected using an ECL Plus western blotting detection system (Amersham, GE-Healthcare, Buckinghamshire, UK), an enhanced chemiluminescence detection system.
6. Statistical analysis
Differences in each variable between patients and controls were evaluated with Mann-Whitney U-tests and a Wilcoxon test. A p-value less than 0.05 was considered statistically significant.
Results
1. NTM leads to the phosphorylation of MAPKs in monocytes of patients with M. abscessus lung disease, but expression of MAPKs in patients is less than that of healthy controls
Because NTM-induced expression of MAPKs in healthy human monocytes has been confirmed in other studies, we examined whether MAPKs are activated in monocytes of patients with M. abscessus lung disease after stimulation with NTM. We then compared the expression levels of MAPKs in monocytes between the patients and healthy controls.
Western blot analysis with anti-phospho-ERK1/2 in patients showed that ERK1/2 activity after M. avium stimulation (MOI 1:70) was upregulated as compared to ERK1/2 in the non-stimulated state (p=0.018) (Figure 1A). ERK1/2 expression after LTA showed similar results (p=0.043), although the expression of ERK1/2 in patients was lower than that of healthy controls in response to M. avium stimulation (p=0.010), despite the small difference in ERK1/2 expression during the non-stimulated state between the patients and healthy controls (Figure 1A). Similar profiles were observed with response to p38 activation between patients with M. abscessus lung disease and healthy controls (Figure 1B).

Mycobacterium avium-induced extracellular signal-regulated kinase (ERK1/2) and p38 expression in peripheral blood monocytes from patients with M. abscessus lung disease and healthy controls. ERK1/2 (A) and p38 (B) activation with M. avium or lipoteichoic acid (LTA) significantly decreased in patients (gray bar) as compared to healthy controls (white bar). Expression of ERK1/2 and p38 via inhibition with the anti-TLR2 antibody were not different between patients and controls. *p<0.05. †p<0.01. TLR2 Ab: Toll-like receptor 2 antibody.
After inhibition with a TLR2 neutralized antibody in healthy controls, expression of ERK1/2 after M. avium stimulation was lower than ERK1/2 without TLR2 inhibition (p=0.018). However, it did not differ significantly from ERK1/2 activation in the patients after TLR2 inhibition with the antibody (Figure 1A). Thus, the expression of ERK1/2 in response to M. avium stimulation with TLR2 inhibition was not different between the patients and controls, in contrast to significant differences of ERK1/2 between patients and controls after M. avium stimulation without TLR2 inhibition (Figure 1A). The expression of p38 showed a similar tendency (Figure 1B).
2. NTM-induced cytokine production in human monocytes is dependent on ERK1/2 and p38, but lower cytokine levels were observed in patients with M. abscessus lung disease as compared to healthy controls
To determine whether MAPK activation was necessary for NTM-induced cytokine production, human monocytes were pretreated with the ERK1/2 inhibitor PD98059 or the p38 inhibitor SB203580 prior to M. avium stimulation.
In human monocytes from healthy controls, TNF-α secretion significantly increased after M. avium stimulation (MOI 1:70) as compared to the non-stimulated state (p=0.018). In contrast, inhibition of ERK1/2 or p38 reduced TNF-α production by M. avium stimulation (Figure 2A). Similar results were obtained with IL-6 production (Figure 2B). Moreover, IL-10 production after M. avium stimulation was suppressed by the inhibition of p38, but not the inhibition of ERK1/2 in healthy controls (Figure 2C).

(A~C) Inhibitory effects of extracellular signal-regulated kinase (ERK1/2) and p38 on Mycobacterium avium-induced tumor necrosis factor (TNF)-α, interleukin (IL)-6, and IL-10 in monocytes from patients with M. abscessus lung disease and healthy controls. The anti-TLR2-specific antibody, the p38 signaling inhibitor SB203580 (SB), or the ERK1/2 selective inhibitor PD98059 (PD) prior to infection with M. avium at a MOI of 70 was added to the cells. The supernatants were harvested and ELISA was used to measure cytokine activity. *p<0.05. †p<0.01. TLR2 Ab: toll-like receptor 2 antibody; MOI: multiplicity of infection; ELISA: enzyme-linked immunosorbent assays; controls: white bar; patients: gray bar.
We compared cytokine production in monocytes from patients with M. abscessus lung disease versus healthy controls in the presence and absence of ERK1/2 or p38 inhibition followed by M. avium stimulation. TNF-α secretion in response to M. avium stimulation was lower in patients as compared to the controls (p=0.003). However, M. avium-induced TNF-α production after blocking ERK1/2 or p38 pathway did not show significant difference between patients and controls (Figure 2A). A similar tendency was shown in IL-6 (Figure 2A) and IL-10 (Figure 2C).
Discussion
To the best of our knowledge, the current study is the first to examine MAPK expression in patients with NTM lung disease including M. abscessus lung disease. The present data demonstrate that both M. avium and LTA induce p38 and ERK1/2 expression in monocytes from healthy controls, and subsequently upregulate TNF-α, IL-6 and IL-10 production. However, in monocytes from patients with M. abscessus lung disease, the induction of p38 and ERK1/2 expression, and TNF-α, IL-6, and IL-10 production, occurred to a significantly lesser extent. IL-10 production is related not only to p38 but also to the ERK1/2 pathway. Thus, current findings suggest that impaired induction of p38 and ERK1/2 expression in response to M. avium or LTA stimulation may contribute to host susceptibility to M. abscessus lung disease. For tolerance effect is partly eliminated, M. abscessus primed cell is stimulated by M. avium instead of same strain.
Since NTM are ubiquitous organisms, most people are resistant to infection unless their defense mechanisms have undergone iatrogenic alteration. However, the nature of the precise immune dysfunction that predisposes otherwise healthy subjects to NTM lung disease are not clear. A few studies that have compared the immune responses of PBMCs from patients with NTM lung disease and healthy controls have shown that patients produce lower concentrations of IL-12, interferon-γ, and TNF-α25-28. These results suggest that susceptibility to NTM lung disease is related to the suppression of the T-helper cell (Th) type 1 immune responses. Downregulation of TLR2 was suggested to be involved in the immune suppression of NTM disease26. However, additional detailed mechanisms responsible for this immunologic imbalance remain unknown.
MAPK is involved in cytokine responses and inflammation linked to the engagement of TLR2 and myeloid differentiation factor 88 as demonstrated for NTM13,16,29. The present Western blot data show that p38 and ERK1/2 expression decreases with inhibition by the TLR2 antibody. These findings suggest that MAPK signaling pathway is related to the TLR2 pathway.
TNF-α is thought to mediate pathologic inflammatory reactions and protective responses to mycobacterial infections and to play a central role in granuloma formation, both directly and through the recruitment of chemokines30. Although IL-6 has been shown to promote the intracellular growth of mycobacteria in mononuclear cells31,32 IL-6 seems to be critical in resistance to mycobacterial infection33. Therefore, down-regulation of these cytokine in human with mycobacterial infection leads to disease development. In this study, TNF-α and IL-6 secretion decreased following stimulation with M. avium and LTA when pretreated with p38 inhibitor and ERK1/2 inhibitor. These findings strongly suggest that p38 and ERK1/2 play essential roles in the production of TNF-α and IL-6 against M. avium. Previous studies have revealed that TNF-α, IL-6, and IL-10 production in M. avium or M. abscessus infection are increased by activation of the p38 and ERK1/2 MAPK signaling pathway in PBMCs of healthy humans12. M. abscessus was demonstrated to be activated by the p38 and ERK1/2 MAPK pathways and induces the secretion of TNF-α, IL-6, and IL-12 p40 via TLR2 in murine macrophages13. Some studies have indicated that p38 and ERK activation are required for mycobacteria-induced TNF-α secretion17,34,35.
IL-10 is an anti-inflammatory cytokine mostly produced by Th2 cells. Previous studies have shown that Th2 immune responses might increase in NTM lung disease since IL-10 is higher, whereas other cytokines are lower in patients with NTM lung disease25,28. However, the present data showed that IL-10 production was lower in patients with NTM lung disease than healthy controls and it decreased significantly with inhibition of p38 signaling. These findings suggest that the ERK1/2 and p38 MAPK pathways are critical for M. avium-induced TNF-α and IL-6 formation, whereas only the p38 MAPK pathway is essential for M. avium-induced IL-10 production. Recent studies have found that IL-10 was greatly reduced (>90%) by the p38 inhibitor, whereas the ERK1/2 inhibitor only partially interfered with IL-10 (35~45%) in study on healthy human monocytes stimulated with M. avium or M. abscessus12. Another study of human macrophage stimulated with M. avium showed that induction of IL-10 was critically dependent on p38 MAPK activity, but only partially dependent on the ERK1/2 pathway36. Such divergent requirements for the MAPK pathway of TNF-α and IL-10 might affect regulation of production of inflammatory and anti-inflammatory cytokine in NTM infection, although further study of type of cell or another strain is requirement. Furthermore, this different MAPK role of TNF-α and IL-10 will be considered for the usage of MAPK pathway of novel target therapy.
Although these findings strongly suggest that regulation of the p38 and ERK1/2 MAPK pathways may be an important determinant of NTM infection susceptibility, the relationship between NTM lung disease and MAPK and cytokine expression was not fully examined. In the present study, p38 and ERK1/2 MAPK expression, and TNF-α, IL-6, and IL-10 production in monocytes in NTM lung disease were lower than in healthy controls. In addition, treatment with the inhibitor of p38 or ERK1/2 blocked M. avium induced cytokine production in monocytes of healthy controls, but only had a minimal effect in those of patients. These results indicate that defects in the MAPK pathway are a crucial cause for the reduction in cytokine production during NTM lung disease. The present study has several important limitations. First, the sample size in this study was relatively small, perhaps too small to make a definite conclusion. Therefore, the result of this study has value of preliminary study. In addition, peripheral blood monocytes can reflect the immunoreactivity of airway cells, but the immune response of peripheral blood monocytes may be confounded due to a lack of local immunoregulatory mechanisms present in the lung37,38. Therefore, further studies involving MAPK expression and subsequent cytokine responses using bronchoalveolar lavage cells will be needed. Finally, depression of MAPK expression and subsequent downregulation of cytokine responses in patients with NTM lung disease might be a secondary phenomenon of NTM infection, and is not attributable to the susceptibility of patients with the disease. Secondary phenomenon is that impairment of immune response or tolerance effect for stimulation from other infection coming out after NTM infection. Therefore, further studies are needed to examine MAPK expression and cytokine responses before and after treatment of M. abscessus infection.
NTM infection induced p38 and ERK1/2 expression in monocytes from healthy controls and subsequently upregulated TNF-α and IL-6 production. IL-10 production was related to the p38 pathway, but not the ERK1/2 pathway. In monocytes from patients with M. abscessus lung disease, however, the induction of p38 and ERK1/2 expression, and the production of TNF-α, IL-6, and IL-10 were significantly lower. These findings suggest that decreased activity of MAPK and cytokine secretion in monocytes from patients with M. abscessus lung disease may partially explain the reasons for host susceptibility to these uncommon infections.
Acknowledgements
This work was supported by the Mid-career Researcher Program through an NRF grant funded by MEST (2010-0027659) and IN-SUNG Foundation for Medical Research (CA 98051).