


Introduction
Chronic cough is the most common disease in respiratory specialty and community clinics that impairs quality of life (QoL) and increases the economic burden1,2. The common underlying causes associated with chronic cough included asthma syndromes, gastroesophageal reflux disease, upper airway disorders, and various combinations of these diseases3. Although most patients are treated effectively, cough can persist even after extensive examination or treatment trials in some outpatients. These patients are diagnosed as unexplained chronic cough, idiopathic cough, or refractory chronic cough when there is no identifiable cause4,5. This is always a considerable challenge in clinical practice. Considering the significant medical burden of cough, it is important to establish more effective treatment of patients, especially with chronic cough.
A major hindrance for the development of chronic cough treatment is inadequate understanding of the pathophysiological mechanism of cough. Although it is induced by a variety of stimuli, cough reflex is mediated by the vagal primary afferent nerve that is distributed in the bronchial tree6 and in the extra visceral areas (main bronchus, trachea, and larynx)7. It is widely accepted that the sensitivity of the cough reflex is increased in chronic cough8,9. Meanwhile, more and more evidences showed that the sensory disorder of the laryngeal branches of vagus nerve is an important pathogenetic mechanism10,11,12,13,14,15,16,17,18. As pain and cough share the remarkably similar pathways, gabapentin, traditionally used in treatment of neuropathic pain, was recently used as a non-specifc antitussives for chronic idiopathic cough15,17,19.
Gabapentin has a similar lipophilic structure to the neurotransmitter gamma aminobutyric acid which notoriously performs central action20. Accordingly, it may also cause central nervous system side effects in the patients taking it. Systematically evaluating the evidence regarding the use of gabapentin medications in the treatment of refractory chronic cough cases may provide views about their efficacy and a better understanding of the studies related to this new therapeutic strategy. Current study is limited by a relatively small sample size, and there was no systematic review of studies regarding gabapentin antitussive therapies. Therefore, our systematic review was conducted to examine the articles concerning the use of gabapentin in the management of chronic cough. We performed the present systematic review to objectively assess the safety and efficacy of gabapentin in chronic cough so as to provide valuable references for clinical medication.
Materials and methods
1. Data sources and literature search strategy
Data searching were performed using PubMed, Embase, CBM, and Cochrane Library database by two authors independently, from their dates of inception to 1 July 2017. No language and geographical restriction was imposed. We translated non-English publications into English when they were satisfied for inclusion criteria. Search keywords used included: (cough or bronchitis or respiratory tract infections or irritable larynx or pharyngeal diseases or laryngeal diseases or postviral vagal neuropathy or central sensitisation) and (neurontin or gabapentin or gralise or neuromodulator). Unpublished data or data derived only from abstracts were not used. We also searched reference lists of all primary studies and review articles.
2. Inclusion and exclusion criteria
We used following inclusion criteria to select studies for the systematic review: (1) adults with chronic cough of unknown etiology at least 8 weeks' duration, (2) purpose of the use of gabapentin for the treatment of cough, and (3) outcome measures standard should be inclued. Exclusion criteria are as follows: (1) patients younger than 18 years; (2) nonhuman studies; (3) cough due to clear etiology like reflux disease, sinonasal pathology, allergy, pulmonary diseases, angiotensin-converting enzyme inhibitors (ACEIs) and so on; (4) studies with unclear or incomplete information.
3. Outcome measures
One or more of the following outcomes should be included: cough severity score, Leicester Cough Questionnaire (LCQ), visual analogue scale (VAS), QoL, cough severity, cough frequency, clinician assessment, urge-to-cough score, and laryngeal dysfunction score.
4. Data extraction and quality assessment
Data were selected and extracted from all of the included studies independently by two authors. Each study was noted by the major information including the reference, country, year of publication, study type, number of participants, patient age, medication regimen, follow-up time, inclusion and exclusion criteria of study, definition of effective treatment, and medication adverse effects. Two reviewers independently evaluated each relevant article and reached agreement for study inclusion. The quality of each trial was assessed by the following trial design features: (1) consecutive status of patients for non randomized controlled trails, (2) type of study outcome, (3) whether study outcome was chosen a priori, and (4) exclusion/inclusion criteria for patient enrollment. Owing to the limited numbers of studies, variability in the quality of researches, and inconsistent reporting of outcomes, no metaanalysis was attempted.
Results
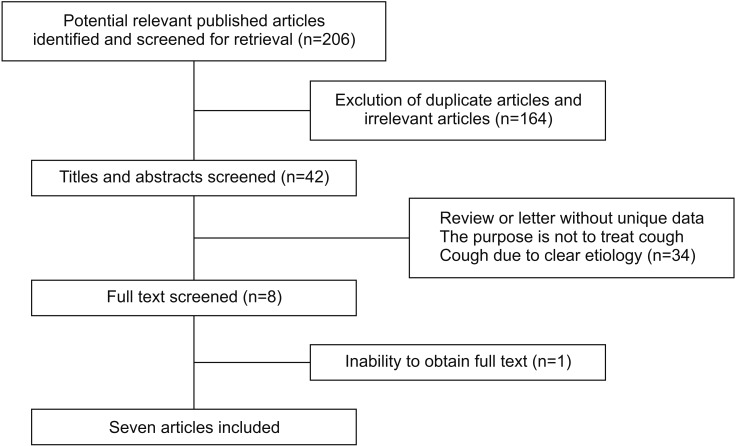
Initial data search identified a total of 206 potentially relevant articles (Figure 1). We removed 30 duplicated articles and excluded 134 after screening the title and abstracts. After reviewing the full-text articles, 34 studies were excluded, mainly because they were reviews and letters without new data or were not satisfactory for the study selection; one study was not included because of the inability to obtain full text21; we included one article which was a case report about evidence for chronic cough as a sensory vagal neuropathy, owing to it was also a cause of refractory chronic cough18; a study published in China was also included as it was a relatively complete randomized controlled trials (RCTs)22; eventually, all together seven papers were selected for further analysis, and a detailed description of these studies is provided (Table 1).
Among these two studies were placebo controlled RCTs17,22. The RCTs were placebo controlled, one study participants and researchers were blinded (investigators evaluating the outcome were not blinded)17, and the other did not reported blind method22. One study was a prospective case series design of consecutive patients14; two studies were retrospective trails23,24, one was a retrospective cohort of consecutive patients, consecutive status in the other retrospective case series was not reported. The rest of the two studies were a case report of two patients consist of one male and one female and a case series of six participants whose consecutive status were not clear6,15. Two studies from same authors were funded by the National Health and Medical Research Council of Australia6,17. The rest of the studies did not describe the financial support. All of the studies included patients with cough for at least 8 weeks (Table 2).
The inclusion/exclusion criteria adopted by the investigators included a negative response to empirical treatment trials with proton pump inhibitors, inhaled corticosteroid, oral corticosteroid or nasal corticosteroid treatment6,21,22; normal spirometry6,21; smoking17; modified barium swallow, computed tomography (CT), magnetic resonance imaging (MRI), pH testing14; gastroesophageal reflux disease and asthma15,17,23.
In the research of Lee and Woo14, most of the patients had received previous treatment and examination, including the treatment of gastroesophageal reflux disease, modified barium swallow, CT, MRI, and pH monitoring, but it was unclear whether these had been systematically carried out in all patients. In the study by Mintz and Lee15, all patients were treated initially with corticosteroids therapy, not every patient had been evaluated for postnasal drip but did have prior empirical reflux treatment trials and surveys for pulmonary disease in some way. Only an RCT designed by Ryan et al.17 mentioned smoking and ACEI as inclusion criteria.
Different outcome criteria were used to evaluate the clinical therapeutic effect of gabapentin (Table 3). The two RCTs used LCQ instruments, VAS and an objective cough monitor to determine cough frequency17,22. Two studies categorized treatment response based on self-reported percent improvement. A study by Lee and Woo14 simply referred to the improvement of clinical symptoms (yes or no), and if the system response was reported by patient's self-reported or physician assessment was not clear15. A cough severity score, which was correlated with the average of the four LCQ scores, was performed by Van de Kerkhove et al.23. Mintz and Lee15 evaluated the symptom response using clinician reports15. One RCT by Ryan et al.17 also used capsaicin cough challenge as a measurement to evaluate objective outcome, in which participants' cough threshold was assessed in response to the chemical tussive capsaicin.
Gabapentin treatment improved symptoms of cough17. In the two RCTs improvements were seen in cough-specific QoL (LCQ score), cough severity (VAS score), and there was a reduction in cough frequency17,22. The RCT using capsaicin cough challenge showed that capsaicin cough reflex sensitivity did not change significantly with gabapentin treatment17. One study showed the rate of treatment response was 68% using a binary rating of improvement, compared with 80% in the patients with demonstrable findings of laryngeal neuropathy, while patients without evidences of motor neuropathy had only a 37.5% response rate14. In the study using clinician assessment response, half of the patients had complete remission and the remaining patients had improved to varying degree in cough15. One RCT study also evaluated clinical symptom improvement time and found the onset of action of gabapentin was within 4 weeks, and the treatment effect was maintained with maximal dosing during 8 weeks17. Mintz and Lee15 noted the duration of improvement ranged from 6 months to ongoing. The improvement in cough-specific quality of life was not sustained after discontinuing gabapentin and the LCQ score returned to baseline values17. A similar trend was also found in cough severity and cough frequency.
Adverse effects may come from gabapentin treatment of chronic cough. Reported side effects included fatigue, dry mouth, drowsiness, and dizziness14,15,17,22,23. Rates of patient-reported side effects in chronic cough patients ranged from 40% to 18% with varying degrees of severity14,15,17,22,23. In two studies, side effects was not reported6,24. One RCT found side effects in 31% of gabapentin group while 10% of patients taking placebo, including confusion, dizziness, nausea, dry mouth, fatigue, headache, blurred vision, and memory loss17. The other RCT reported adverse events in 40% of gabapentin group vs 23.1% in the placebo group, with similar side effects as Ryan et al.17 reported.
Discussion
This systematic review sought to examine evidence for efficacy and safety of gabapentin in the treatment of chronic cough. We examined the data in the current studies regarding this management strategy. There were considerable distinctions in the quality and type of studies on the treatment of chronic cough, which used gabapentin of interest. Although two RCTs were included, the quality of one study left much to be desired, and owing to the limited numbers of participants, calculation couldn't be evaluated comprehensively17,22.
The other researches included one non-controlled prospective case series of consecutive participants14, one non-controlled retrospective cohort of consecutive cases23, one retrospective case series24, and two case reports whose consecutive status is unknown6,15. Even though all included researches involved adults with chronic cough of unknown etiology at least 8 weeks' duration, there were considerable variations between preliminary investigation and previous therapy trails in these studies. Potential heterogeneity may be derived from the exclusion of some particular diagnoses, such as reflux or asthma.
Although different outcome measures were used, it was observed which benefited from gabapentin. Patients experienced improvements were seen in lower LCQ score, VAS score, and a reduction in cough frequency6,17,22,23. Additionally, over 68% cases obtained some treatment response, and more than 80% had a reduction in varying degrees in symptoms of cough14,15,22,23,24. Nevertheless, there remain some problems, in the case of the optimum dose, treatment duration, time to the best benefit, and symptom reduction rates after therapeutics. Unfortunately, only one RCT reported treatment response, which observed no improvement continuously in cough-specific quality of life after discontinuing gabapentin and the LCQ score returned to baseline values. This may indicate long-term maintenance therapy is suitable for refractory chronic cough, which should be examined by further studies. The neuromodulatory effect of gabapentin on central sensitisation (CS) was noted by one RCT, which reported patients in the treatment group with CS symptoms had noticeable improvements in LCQ score vs those without symptoms of CS17. Lee and Woo14 reported higher treatment response rate in the patients with demonstrable findings of laryngeal neuropathy than patients without evidences of motor neuropathy. A case report noted that both refractory chronic cough patients with Arnold's nerve reflex hypersensitivity were successfully treated with gabapentin6. Laryngeal irritability, such as laryngospasm and throat clearing, was attributable to cases with additional symptoms14,24. In addition, Madanick et al.21 reported cases seen in a tertiary care esophageal clinic for esophageal diseases and swallowing for chronic cough that the symptoms improved in most patients with a low-dose gabapentin, no matter the results of reflux testing. Further researches about these subgroups may provide more useful information about the gabapentin treatment on these type-specific patients.
Side effects such as fatigue/drowsiness/dry mouth/lethargy and dizziness generated early and alleviated voluntarily within a short period in the majority of patients, and only a few patients withdraw because of adverse effects17,22. Gabapentin in overdose often generates mild toxicity with clinical presentations without the need for medical treatment25,26. Further investigation into gabapentin long-period security, optimum dose, treatment duration is necessary.
There are variations on the design of study, quality of studies, medical intervention, dosage, and outcomes in included articles. Owing to these inconsistencies, a formal metaanalysis was not conducted. This systematic review showed superior efficacy and a good safety compared with placebo or standard medications in the use of gabapentin for patients with chronic cough, and further more RCTs are needed.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






