Current Chronic Obstructive Pulmonary Disease Treatment Status in Asia: A Position Statement of the Asian Pacific Society of Respirology
Article information

Chronic obstructive pulmonary disease (COPD) is known as a major disease which poses substantial socioeconomic burden especially in Asia [1]. Although the Global Initiative for Chronic Obstructive Lung Disease (GOLD) document recommends how to treat COPD patients, there has been no universal Asian recommendation [2]. Also, economic status varies in Asian countries and the medical system is heterogeneous. Thus, it is expected that COPD treatment status in Asia would be very heterogeneous. However, there have been few publications that have analyzed and compared clinical characteristics and treatment status in Asia. The purpose of this study is to describe clinical characteristics and current medical treatment status of COPD in Asia Pacific countries.
This was a cross-sectional study that analyzed treatment status of COPD in four Asia Pacific countries; South Korea, Japan, Indonesia, and Australia. Data on South Korean COPD patients were extracted by the Korea COPD Subgroup Study (KOCOSS) database, a nationwide multicenter cohort of South Korean COPD patients [3]. Japanese data were collected by COPD Assessment in Practice (CAP) study, a multicenter cross-sectional study that enrolled clinical diagnosis of COPD patients who have not experienced exacerbation in a previous month [4]. Indonesian data were collected by the outpatient clinic at Phersahabatan General Hospital. Also, Australian data were previously published claims data extracted from the Australian Government Department of Veterans’ Affairs (DVA) [5]. Baseline characteristics including age, sex, smoking history, and body mass index (BMI) were collected. Additionally, clinical characteristics associated with COPD including lung function test results, COPD Assessment Test (CAT) scores, history of exacerbation in previous year, and pharmacologic regimens were evaluated.
Table 1 summarizes the differences in clinical characteristics of COPD patients between Asian countries. COPD patients in Australia were relatively older and more likely to be female, compared to other countries. The proportion of never-smokers was highest in Indonesia, and least in the Japanese COPD population. Results of lung function tests also showed heterogeneous results. Post-bronchodilator forced expiratory volume in 1 second was lowest in Indonesians, followed by Japanese and South Koreans. The total CAT score was higher in South Korean patients com pared to Indonesian patients, and a history of exacerbation in the previous year was highest in Indonesian patients. Long-acting muscarinic antagonist (LAMA) were most frequently used in Australia, but used in only 2.7% of patients in Indonesia. Triple therapy was most frequently used in Japan and South Korea, and least used in Indonesia. In contrast, inhaled corticosteroid plus LABA combination agents were most frequently used in Indonesia, and least used in South Korea.
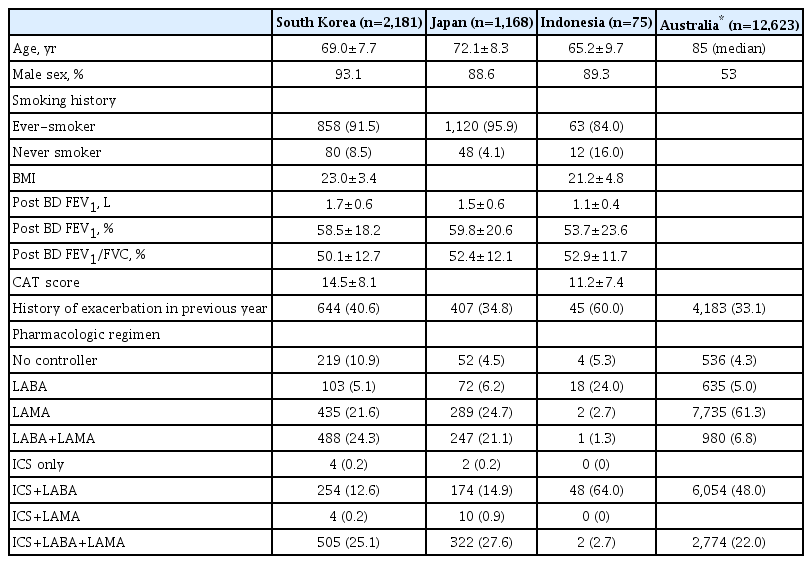
Clinical characteristics of COPD patients in Asian countries
As shown in the present analysis, there was heterogeneity in clinical characteristics and treatment between Asian countries. There were some notable differences in age, sex, smoking history, lung function, CAT score, exacerbation rates, and use of pharmacologic agents. In this study, most of the COPD patients were male, except for Australia, for which nearly half of the patients were female. One of the most important reasons for this difference may be gender difference of the smoking rate between the countries. In the World Health Organization (WHO) report of 2019, gender difference of tobacco use was greater in Asian countries compared to most of the European countries and the United States [6]. In this report, there were relatively similar smoking rates between males and females in Australia (13.8% vs. 10.7%, respectively), which may explain the similar gender difference of COPD prevalence in Australia in our study. Also, DVA provides care to veterans as well as their widows, which may also explain the higher proportion of females with COPD in this data. Previous studies have also reported that the proportion of females among COPD patients was mostly low in Asian countries compared to other regions [3,7-9].
In this analysis of clinical characteristics associated with COPD, lung function was worse in Indonesia, compared to South Korea and Japan. As poor lung function is one of the most important risk factors for exacerbation, the proportion of patients who experienced an exacerbation in the previous year was highest in Indonesia, compared to other countries [10]. Also, relatively lower BMI may have affected frequent exacerbation in Indonesian patients [11]. However, relatively lower CAT score in Indonesia despite poor lung function should be investigated in further studies. There were major differences in medication use between the countries. The differences in the data collection timelines, the local guidelines, the cost of the inhaler, and physicians’ awareness may be associated with these differences.
There were some limitations relative to this study. First, the methods of the data collection were heterogeneous between the countries. The enrollment criteria also were diverse between studies. Additionally, in analysis of treatment measures, the percentage of South Korean and Australian data does not add up to 100%, as those studies permitted multiple choices. In contrast, the data of Indonesian and Japan permitted only one answer for the use of drugs, that the percentage add up to 100%. For these reasons, our data may not present definitive results with statistical analysis. Second, COPD patients enrolled in the studies may not represent nationwide COPD patients of each target country. For example, the Indonesian study was a single center study that only enrolled patients who visited the outpatient clinic. Also, the Australian study was based on DVA, which may not represent the general Australian population. Third, although we present differences of prescribed therapies between the countries, it was not possible to identify the appropriateness of the prescription. Finally, the time frames for the patient registration were all different. Despite these limitations, our study may have value in that the data shows prominent heterogeneity between Asian countries, and present importance of further investigations.
In conclusion, we collected medical data of four Asian countries to compare their clinical characteristics and pharmacologic regimen. We reveal herein the clinical heterogeneity and difference of medication use between the Asian countries.
Notes
Authors’ Contributions
Conceptualization: Milne S, Yunus F, Rhee CK, Matsunaga K. Methodology: Choi JY, Milne S, Yunus F, Rhee CK, Matsunaga K. Investigation: Choi JY, Milne S, Yunus F, Rhee CK, Matsunaga K. Writing - original draft preparation: Choi JY. Writing - review and editing: Choi JY, Milne S, Yunus F, Rhee CK, Matsunaga K. Approval of final manuscript: all authors.
Conflicts of Interest
Chin Kook Rhee serves as deputy editor of the Tuberculosis of Respiratory Diseases, but has no role in the decision to publish this article. All remaining authors have declared no conflicts of interest.
Funding
No funding to declare.