Body Mass Index as a Predictor of Acute Kidney Injury in Critically Ill Patients: A Retrospective Single-Center Study
Article information

Abstract
Background
The aim of this study was to examine the influence of body mass index (BMI) on the development of acute kidney injury (AKI) in critically ill patients in intensive care unit (ICU).
Methods
Data of patients admitted to medical ICU from December 2011 to May 2014 were retrospectively analyzed. Patients were classified into three groups according to their BMI: underweight (<18.5 kg/m2), normal (18.5–24.9 kg/m2), and overweight (≥25 kg/m2). The incidence of AKI was compared among these groups and factors associated with the development of AKI were analyzed. AKI was defined according to the Risk, Injury, Failure, Loss of kidney function, and End-stage (RIFLE) kidney disease criteria.
Results
A total of 468 patients were analyzed. Their mean BMI was 21.5±3.9 kg/m2, including 102 (21.8%) underweight, 286 (61.1%) normal-weight, and 80 (17.1%) overweight patients. Overall, AKI occurred in 82 (17.5%) patients. The overweight group had significantly (p<0.001) higher incidence of AKI (36.3%) than the underweight (9.8%) or normal group (15.0%). In addition, BMI was significantly higher in patients with AKI than that in those without AKI (23.4±4.2 vs. 21.1±3.7, p<0.001). Multivariate analysis showed that BMI was significantly associated with the development of AKI (odds ratio, 1.893; 95% confidence interval, 1.224–2.927).
Conclusion
BMI may be associated with the development of AKI in critically ill patients.
Introduction
Body mass index (BMI), calculated from the height and weight of a patient, is a simple and useful index for obesity1. BMI has been reported to be an important prognostic factor for many medical conditions. For example, in chronic obstructive pulmonary disease, chronic renal failure, and cancer, mortality is increased in underweight patients23, whereas in many metabolic diseases, including hypertension, diabetes mellitus, and dyslipidemia, mortality is commonly increased in overweight patients4. Moreover, the relationship between BMI and all-cause mortality in the general population is known to be ‘J’- or ‘U’-shaped5.
Many studies have examined the usefulness of BMI as a prognostic factor in critically ill patients with differing results. Mortality appears to be increased in morbidly obese patients6, while no relationship between mortality and obesity was observed in another prospective study7. Moreover, recent studies have shown that mortality in the intensive care unit (ICU) is lower in obese patients than in those who are underweight789. The development of acute kidney injury (AKI) in ICU patients is a frequent complication that can affect the prognosis1011. Therefore, the development of AKI in these patients and the associated risk factors have been extensively studied11. However, only a few studies have assessed the relationship between BMI and AKI in critically ill patients12131415. Accordingly, the purpose of this study was to assess the influence of BMI on the development of AKI in critically ill patients.
Materials and Methods
1. Study design and settings
All critical-ill patients who were admitted to the medical intensive care unit (MICU) at Gyeongsang National University Hospital (hospital total, 890 beds; MICU, 13 to 15 beds) between December 2011 and May 2014 were retrospectively studied. The admission was decided by attending physician according to general criteria of ICU admission16. Before admission, consents were received from patients' family or caregiver. Patients were excluded if they were admitted for acute coronary syndrome, overdose, acute cerebrovascular disease, and chronic renal failure or were <18 years of age.
This study was approved by the institutional review board of Gyeongsang National University Changwon Hospital (GNUCH-2018-05-014). Informed consent was waived due to the retrospective nature of the study.
2. Data collection and definitions
Demographic information, past medical history, and reason for ICU admission were collected for each patient on admission and discharge from the MICU according to the MICU registry at our institution. The Acute Physiology and Chronic Health Evaluation (APACHE) II score and Sequential Organ Failure Assessment (SOFA) score, measures of severity of illness and predictors of mortality17, were also calculated. Height was recorded based on previous medical records or the ICU admission measurement. Body weight was measured automatically using a calibrated bed scale (VersaCare Bed; Hill-Rom, Batesville, IN, USA) at ICU admission. BMI was calculated as body weight (kg)/height (m2). The patients were classified into three groups based on the degree of obesity as defined by the World Health Organization and the National Heart, Lung and Blood Institute of the National Institutes of Health as follows: underweight (BMI, <18.5 kg/m2), normal (BMI, 18.5–24.9 kg/m2), and overweight (BMI, ≥25.0 kg/m2) groups18.
AKI was defined by the Risk, Injury, Failure, Loss of kidney function, and End-stage (RIFLE) kidney disease criteria using the creatinine level, glomerular filtration rate, and urine output19. The number of days the patient required mechanical ventilation, length of stay (LOS) in the ICU and hospital, and mortality in the ICU and hospital were assessed.
3. Statistical analysis
Continuous variables are reported as the mean±standard deviation. Categorical variables are described as number (%). Differences between groups were compared using analysis of variance, Student's t test, or chi-square test as appropriate. Univariate and multivariate logistic regression analysis was performed to examine the relation between BMI and the factors associated with the development of AKI. Statistical significance was defined as a p-value of <0.05. All data were analyzed using SPSS version 22.0 for Windows (IBM Corp., Armonk, NY, USA).
Results
1. Patient characteristics
A total of 468 patients were analyzed. The average age was 68.6±13.9 years, with a male-to-female ratio of 2:1. The mean BMI was 21.5±3.9 kg/m2 (range, 12.2–39.6 kg/m2). The mean APACHE II and SOFA scores were 18.8±8.8 and 7.9±4.4, respectively. The average LOS was 10.0±18.1 days in the ICU and 25.7±35.8 days in the hospital. The ICU morality rate was 35.8%, with an overall hospital mortality rate of 44.7%. AKI developed in 82 patients (17.1%).
2. Comparison of clinical characteristics according to the BMI groups
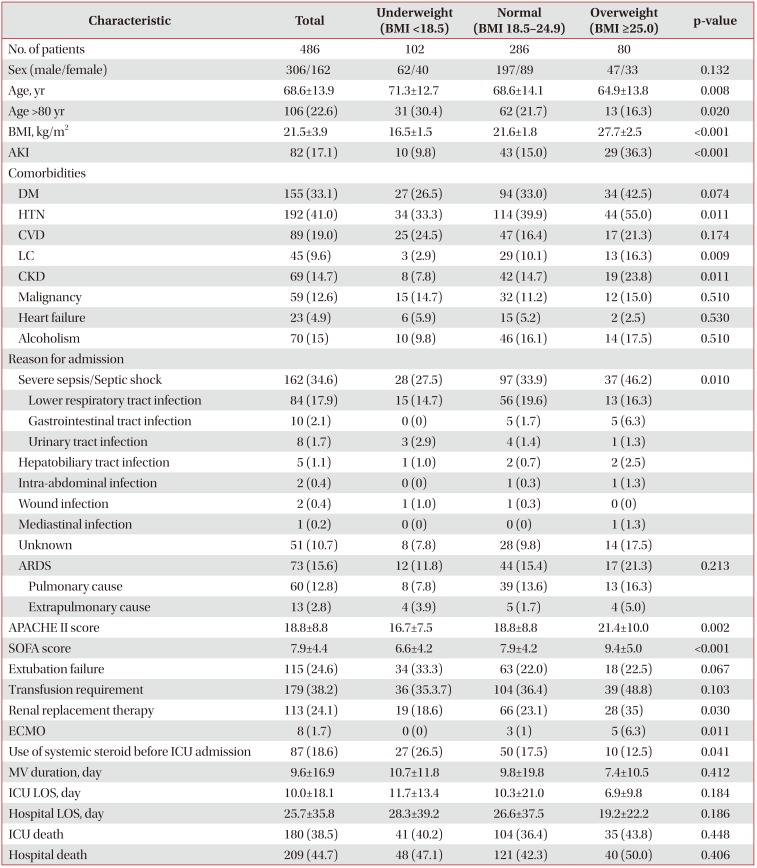
The baseline characteristics of the patients according to BMI group are summarized in Table 1. Of the 468 patients, 102 (21.8%) were underweight, 286 (61.1%) were normal-weight, and 80 (17.1%) were overweight. The mean age of the underweight group was 71.3±12.7 years, which was significantly older than that of the overweight patients (64.9±13.8 years, p=0.008). For the underweight, normal-weight, and overweight groups, the mean BMI values were 16.5±1.5, 21.6±1.8, and 27.7±2.5 kg/m2, respectively. The overweight group had a significantly higher incidence of AKI (36.3%) than the underweight (9.8%) and normal groups (15.0%) (p<0.001 for all). In addition, the overweight group had a higher incidence of hypertension, liver cirrhosis, and chronic kidney disease (p<0.05 for all). The diagnoses on admission included septic shock, acute respiratory distress syndrome (ARDS), gastrointestinal bleeding, with septic shock and ARDS being the main reasons for admission to the MICU. The established causes of septic shock and ARDS were described in the Table 1. Compared to the underweight (27.5%) and normal (33.9%) groups, the overweight group had a significantly higher incidence of septic shock (46.2%) as the reason for ICU admission (p=0.010). The APACHE II and SOFA scores of the overweight group were also significantly higher than those of the other two groups (p=0.002 and p<0.001, respectively). Regarding the clinical outcomes, the LOS in the ICU and hospital tended to be shorter when the BMI was increased. The highest mortality was found in the overweight group, and the lowest mortality was found in the normal weight group. However, there were no significant differences among the three BMI groups regarding the ICU LOS, hospital LOS, ICU death rate, and in-hospital death rate (p>0.05 for all).

Baseline characteristics of patients by BMI groups
3. Comparison of clinical characteristics according to development of AKI
The BMI was significantly higher in patients with AKI than in those without it (23.4±4.2 kg/m2 vs. 21.1±3.7 kg/m2, p<0.05). Patients with AKI had a higher incidence of liver cirrhosis, diabetes, chronic kidney disease, and alcoholism. Moreover, these patients showed a higher incidence of septic shock and ARDS than patients without AKI at the time of admission. Extubation failure, need for transfusion, use of renal replacement therapy, and application of extracorporeal membrane oxygenation were also more common in patients with AKI than in those without it. Regarding the clinical outcomes, the LOS in the ICU and hospital were significantly longer for patients with AKI than for those without AKI (p<0.05). The ICU and hospital mortality rates were also significantly higher in patients with AKI than in those without it (74.4% vs. 30.8% for ICU mortality; 74.4% vs. 38.3% for hospital mortality; p<0.05 for both) (Table 2).

Baseline characteristics according to development of AKI
4. Risk factors for development of AKI
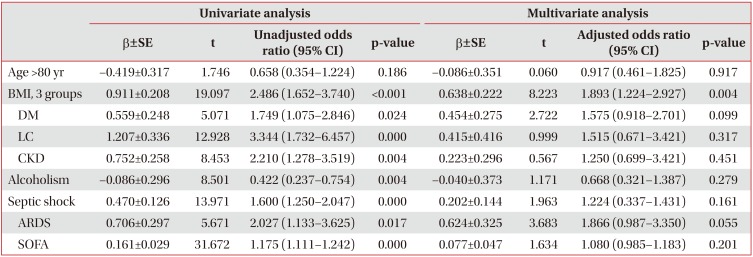
Finally, we assessed the risk factors for AKI in the ICU by logistic regression analyses. In univariate analysis, BMI, diabetes, chronic kidney disease, liver cirrhosis, alcoholism, septic shock, ARDS, SOFA score, and APACHE II score were found to be risk factors for AKI. However, BMI groups were found to be significantly associated with a risk of developing AKI in the multivariate analysis (odds ratio, 1.893; 95% confidence interval, 1.224–2.927; p=0.004) (Table 3).

Univariate and multivariate logistic regression analysis for factor associated with development of AKI
Discussion
This study revealed that BMI was an independent risk factor for the development of AKI in critically ill patients.
Although BMI has been shown to be a useful prognostic marker in critically ill patients, the relationship between BMI and the development of AKI has not been extensively investigated in the literature12131415. However, several reports investigated the association between BMI and the development of AKI in critically ill patients. Soto et al.13 retrospectively analyzed risk factors for AKI in 751 patients with ARDS. The study showed that the prevalence of AKI increased significantly with increasing weight. In addition, there was a 2-fold increase in the risk of AKI in obese patients compared to those of normal weight. The study also reported that the risk could not be completely explained by the severity of illness. A study of 390 patients with sepsis also showed that BMI was higher in patients with AKI than in patients without AKI15. Another study showed the incidence of AKI in patients requiring renal replacement therapy went up as BMI increased12. Further, several studies have reported that AKI develops more frequently in patients with a high BMI after cardiac and abdominal surgery2021. These findings, along with our study, showed that a high BMI was a risk factor for the development of AKI in critically ill patients.
The association between high BMI and risk of AKI development could be explained by several mechanisms. First, obesity causes some hemodynamic changes in the glomerulus such as glomerular hyperperfusion and hyperfiltration due to impaired natriuresis-associated activation of the renin and angiotensin system. Glomerular hyperperfusion and hyperfiltration may be result in glomerular injury. These changes have been demonstrated in an experimental animal model of obesity and in obese patients2223. Second, obesity can increase the hemodynamic and metabolic load on each individual glomerulus, which results in a low number of functional nephrons in obese patients24. In turn, a low number of functional nephrons was related to glomerular hypertrophy and glomerulosclerosis due to increased capillary pressure on the remaining functional nephrons24. Third, adipocytes may be as a production site for activated inflammatory cytokines and oxidative stress in obese patients25. Increased oxidative stress can contribute to detrimental changes in the glomeruli26. Taken together, in obese type II diabetes mellitus patients, reduction of body weight has been shown to be associated with significant decreases in proteinuria. This finding support that harmful influence of obesity to kidney injury27.
Liver cirrhosis and diabetes were more common in patients with AKI than in patients without AKI in our study. In patients with liver cirrhosis, the development of AKI has been shown a relatively frequent problem, especially in critically ill patients, and it has a great impact on prognosis in these patients28. Although diabetes and the development of AKI was not studied in critically ill patients, a recent report showed that, in patients with sepsis, underlying diabetes was not associated with the development of AKI29. Further study is needed to evaluate diabetes as a risk factor for AKI in critically ill patients.
Extubation failure was more common in patients with AKI than in patients without AKI in our study. Extubation failure is usually associated with a longer duration of mechanical ventilation and ICU stay30. It may increase the risk of several complications in the ICU. As a result, ICU patients with extubation failure may be more vulnerable to developing AKI. Previous reports have showed that the time to extubation may be associated with development of AKI in postcardiac surgery patients3132. These reports suggest that the duration of positive pressure ventilation in critically ill patients is an important risk factor for AKI development. In fact, mechanical ventilation itself has been shown to induce proinflammatory reactions and extrapulmonary end organ injury in animal models of mechanical ventilation3334. Conversely, AKI may be associated with a higher rate of extubation failure and delayed weaning.
Although there are conflicting results between BMI and mortality in ICU patients. It is generally reported that patients with Low BMI have a higher mortality rate than those with normal BMI. A large-population prospective study conducted in Korea showed that low BMI patients has a higher mortality than in patient with normal and higher BMI35. In this study, the mortality rate of patients with low BMI was slightly higher (36% vs. 40%) than the patients with normal BMI although there was no statistically significant in two group.
There are some limitations to this study. First, enrolled patients came from the medical ICU of a single tertiary hospital. The risk factors for AKI in the MICU may differ from those in surgical ICUs. For example, in surgical ICU patients, postoperative AKI due to decreased intravascular volume is a relatively common problem. By contrast, the risk factors for AKI in MICU patients usually include the presence of infection and medications (e.g., antibiotics, vasopressors). Second, the characteristics of the enrolled patients were heterogeneous. Hence, the risk for AKI may be quite different and it depend on the underlying disease and the reason for ICU admission. Therefore, the risk factors for AKI are assessed in a homogenous group of patients such as sepsis or acute lung injury.
In conclusion, compared to low or normal BMI, a high BMI was found to be associated with a higher risk of developing AKI in critically ill patients treated in the MICU in this study. This result suggests that BMI may be associated with the development of AKI in critically ill patients.
Notes
Authors' Contributions: Conceptualization: Kim HC. Methodology: Ju S, Kim HC. Formal analysis: Kim HC. Data curation: Ju S, Lee TW. Software: Ju S, Kim HC. Validation: Ju S, Lee TW, Kim HC. Investigation: all authors. Writing - original draft preparation: Ju S. Writing - review and editing: Kim HC. Approval of final manuscript: all authors.
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.