



Introduction
Aging is a global phenomenon, and the population of older adults is increasing in many countries [1,2]. The World Health Organization (WHO) has indicated that the pace of population aging is significantly faster than in the past [3]. In the year 2020, the number of individuals aged 60 years and older surpassed that of children under the age of 5 years, marked a notable demographic shift. Projections by the WHO suggest that by the year 2050, approximately 80% of older adults will reside in low- and middle-income countries, highlighting the projected concentration of the aging population in these regions [3]. The average life expectancy in South Korea was 83.6 years in 2021, an increase from 62.3 years in 1970 [4]. Moreover, the aging index (the number of older population aged 65 years and above per 100 population aged 0 to 14 years) has increased rapidly from 7.2 in 1970 to 167.1 in 2023, and it is expected to reach 456.2 by 2050 [5]. Considering the current population trends, it is highly likely that South Korea will become a rapidly aging society by 2029 [6].
Globally, the age structure of the population is changing [7-10], especially with more older patients [11]. And it characterized by increased frailty [12,13] and multimorbidity [14,15]. In several countries, including Australia and New Zealand, studies [8,16] have shown that the proportion of patients aged 80 and older admitted to intensive care units (ICUs) is increasing year on year. Similar trends are being observed in the United States [17], where the average age of older ICU patients is increasing, as are the number of disabilities and multimorbidity cases. These demographic changes have important implications for ICU management and resource allocation, and studies [18] in South Korea have also highlighted an increase in female ICU patients. Age is an important factor affecting the survival of critically ill patients [7,10], with an older population being associated with a higher prevalence of chronic conditions and a greater proportion of hospitalizations and ICU care [9]. Therefore, in Korea, a rapidly aging society, we aim to study how the epidemiology and clinical outcomes of older ICU patients have changed over the past decade.
Materials and Methods
1. Study design and patients
This retrospective study was conducted in a 28-bed medical, 26-bed surgical, 13-bed neurological, 14-bed neurosurgical, 16-bed cardiovascular, 15-bed cardiac surgical, 10-bed emergent ICU of a single tertiary medical center in Seoul, South Korea. Dedicated to every ICU are a 24-hour intensivist and a 24-hour resident and/or fellow. The bed capacity, staffing, and admission criteria remained unchanged throughout the study period. The admission criteria for the ICU are provided in Supplementary Table S1.
All patients were enrolled who aged ≥65 years admitted to the ICUs between January 1, 2007, and December 31, 2017. We excluded patients after coronary angiography (CAG), or patients had missing data. All aged patients were categorized into three groups: 65 to 74 years (older [O] group), 75 to 84 years (very older [VO] group), and ≥85 years (very very older [VVO] group).
2. Data collection
All medical data were collected from the electronic medical records. Basic demographic characteristics, reason of admission, duration of hospital stay and ICU stay, diagnosis at ICU admission, need for invasive mechanical ventilation and continuous renal replacement therapy, need of vasopressors during ICU stay, ICU mortality, and in-hospital mortality were analyzed.
3. Ethics statement
This study was approved by the Institutional Review Board of Asan Medical Center (2018-0431) and the requirement for informed consent was waived due to the retrospective nature of the study.
4. Statistical analysis
All statistical analyses were approved by the Academic Clinical Research Operating and Supporting System at Chungnam National University Hospital Biomedical Research Institute. For variables that followed a normal or nearly normal distribution, we reported them as means±standard deviations. These were compared using Student’s t-test when comparing two groups, and analysis of variance (ANOVA) when comparing three or more groups. When ANOVA indicated significant differences, we performed post hoc analyses to determine exactly which groups differed from each other. We used methods such as Tukey’s honestly significant difference, Bonferroni correction, or Scheffé test, depending on our specific research questions and the need to control for type I error. For continuous data that did not follow a normal distribution, we reported medians and interquartile ranges. The Mann-Whitney U test was used for comparisons between two groups and the Kruskal-Wallis test for three or more groups. We presented categorical data as proportions and used Pearson’s chi-squared test or Fisher’s exact test for comparisons, the latter being more appropriate for small sample sizes. In our analysis, a simple linear model was used to assess trends in continuous variables. For categorical variables, logistic regression analysis was used to assess trends. Post hoc ANOVA analysis, which was particularly relevant in our study because of the comparison between three groups, was performed with a significance level of p<0.05. This allowed us to understand not only if, but where the significant differences between the groups were, providing a more nuanced understanding of our data. Subsequently, multivariate logistic regression analyses with backward elimination procedures were performed to obtain adjusted odds ratios (ORs) with 95% confidence intervals (CIs) for factors associated with mortality. All p-values were two-tailed. All statistical analyses were performed using SPSS software version 22.0 (IBM Co., Armonk, NY, USA).
Results
1. Patient characteristics
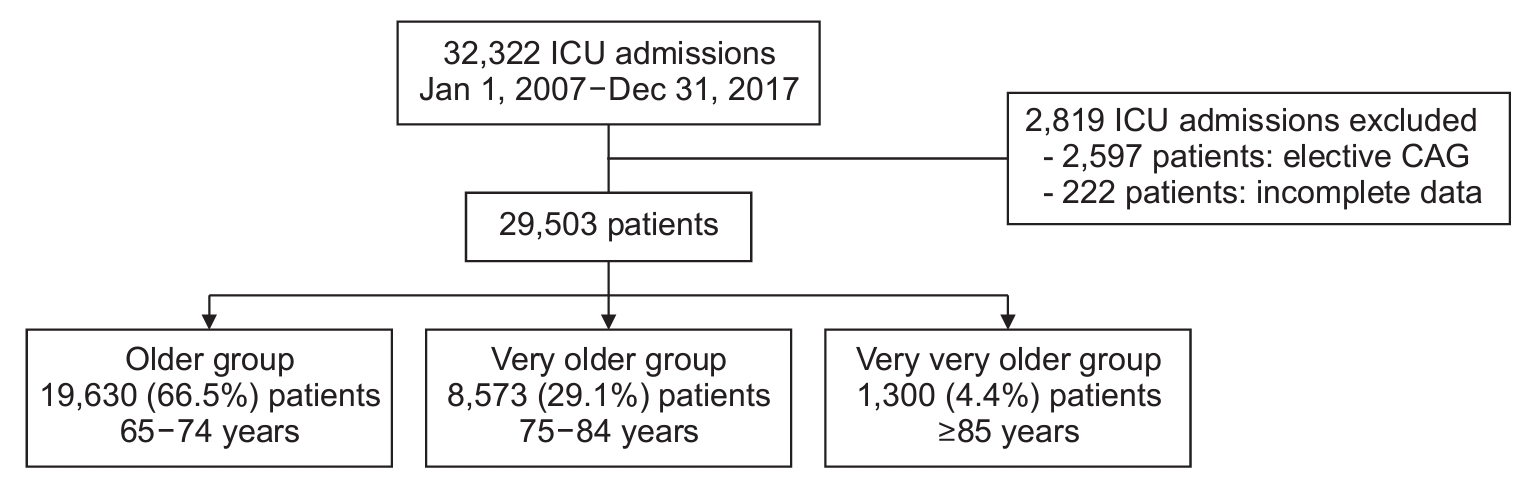
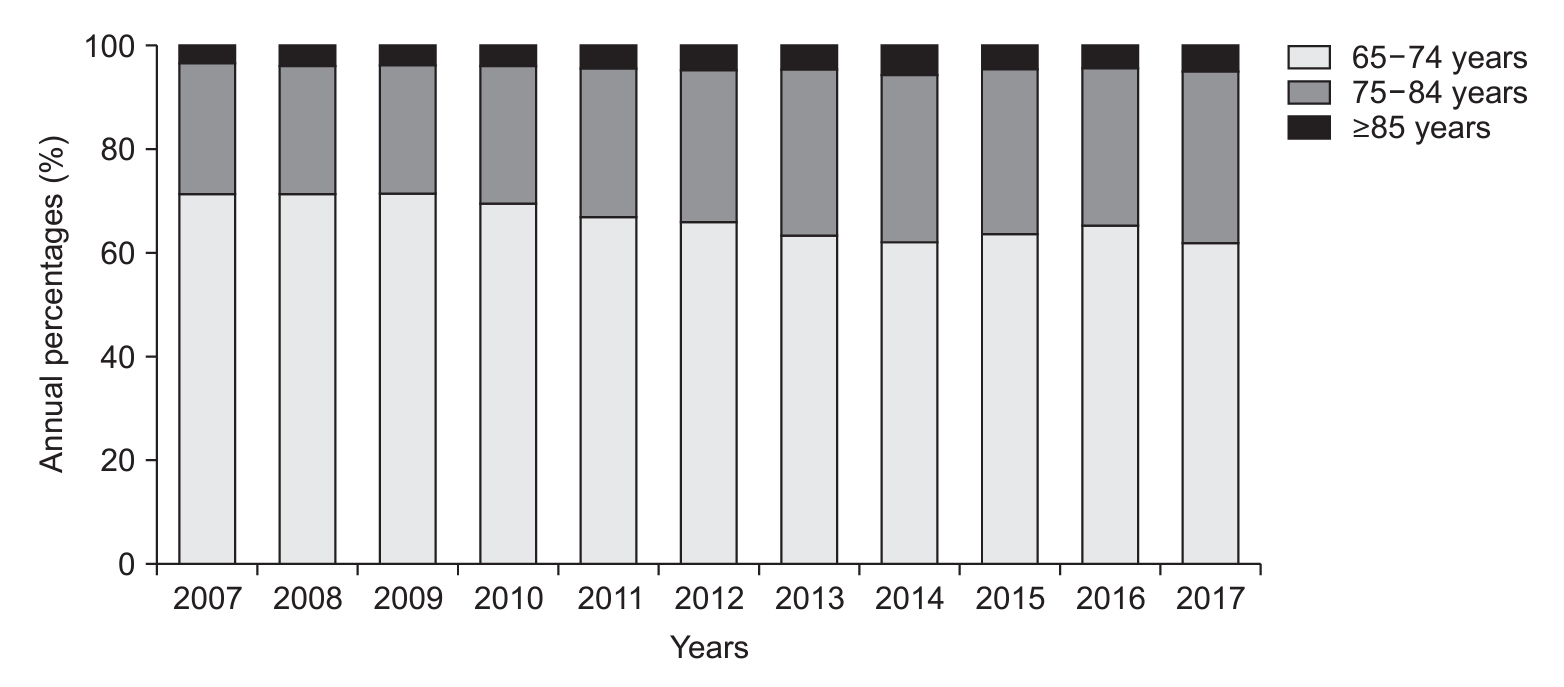
During the study period, there were 32,322 ICU admissions (Figure 1). We excluded patients for observation in the ICU after CAG (n=2,597), or who had missing data (n=222) (Figure 1). The study included 29,503 patients (34.5%) who were older than 65 years. Among these older patients, 19,630 (66.5%) were classified in the O group, 8,573 (29.1%) in the VO group, and 1,300 (4.4%) in the VVO group. In our analysis, we examined the proportions of each group in specific years as well as trends over a 10-year period. Specifically, the proportions for each group were as follows (Figure 2, Supplementary Table S2): For the O group, the proportion was 71.5% (1,666/2,330) in 2007 and decreased to 62.0% (1,930/3,115) in 2017 (p<0.001). For the VO group, there was an increase from 25.2% (586/2,330) in 2007 to 33.0% (1,029/3,115) in 2017 (p<0.001). Similarly, the VVO group showed an increase from 3.3% (78/2,330) in 2007 to 5.0% (156/3,115) in 2017 (p<0.001).
The mean age of ICU admitted patients over the study period increased: 71.9±5.6 years in 2007, and 73.2±6.1 years in 2017 (p<0.001). The number of female patients increased 37.9% (884/2,330) in 2007 and 43.3% (1,348/3,115) in 2017 (p=0.003) (Table 1).
The patient characteristics are shown in Supplementary Table S3. The proportions of male were 60.7% in the O group, 55.6% in the VO group, 47.4% in the VVO group, respectively. As age increased, the number of admissions to the ICU for surgical reasons decreased (p<0.001), and the number of admissions for medical reasons increased (p<0.001). The distribution of diagnosis and surgery at ICU admission differed depending on aged group.
In our analysis of patients hospitalized for medical reasons, we observed statistically significant differences in the prevalence of various diagnoses between the O, VO, and VVO groups. Specifically, the rate of respiratory diagnoses increased from 18.3% in the O group to 21.4% in the VVO group (p=0.005). In contrast, gastrointestinal and hepatobiliary diagnoses showed a significant increase from 6.8% in the O group to 11.3% in the VVO group (p<0.001). Hemato-oncologic diagnoses showed a decreasing trend from 8.7% in the O group to only 1.0% in the VVO group (p<0.001). In the surgical cohort, the types of surgery varied significantly between groups. Gastrointestinal and hepatobiliary surgeries were more common in the VVO group (31.3%) compared to the O group (20.7%) (p<0.001). Orthopedic surgeries showed a significant increase in the VVO group (17.9%) compared to the O group (2.2%) (p<0.001). Neurological surgeries were more common in the O group (22.6%) than in the VVO group (13.4%) (p<0.001). Respiratory procedures decreased from 15.6% in the O group to 4.2% in the VVO group (p<0.001). These findings are detailed in Supplementary Table S3.
When compared to the O and VO groups, noninvasive ventilation, and renal replacement therapy in the VVO group were more frequent, whereas the use of vasopressors was less frequent. The 28 day-ICU mortality and ICU mortality, in-hospital mortality, and ICU length of stay (LOS) were all higher in the VVO group (Supplementary Table S4).
2. Clinical outcomes in the older patients
The ICU LOS was 5.5±9.6 days in 2007, and 4.8±10.1 days in 2017 (p<0.001); hospital LOS was 23.5±44.4 days in 2007, and 17.4±26.2 days in 2017 (p<0.001). In-hospital mortality was 10.3% in 2007 and 7.6% in 2017 (p<0.001), and the ICU readmission rates were 10.8% in 2007 and 7.6% in 2017 (p<0.001) (Table 1).
Table 2 shows the changes in outcomes over the years according to the age groups. Hospital mortality decreased over the study period in all three groups. ICU LOS decreased in the O group and the VO group, while no significant difference was observed in the VVO group. Hospital LOS tended to decrease similarly across all groups.
3. Factors associated with in-hospital mortality
The results of the univariate logistic analysis of factors associated with in-hospital mortality are presented in Table 3. In the multivariate analysis, independent factors of hospital mortality included age (VO group [65-74 years: OR, 1.267; 95% CI, 1.151 to 1.395; p<0.001], VVO group [≥85 years: OR, 2.031; 95% CI, 1.701 to 2.425; p<0.001]), male (OR, 1.200; 95% CI, 1.096 to 1.314; p<0.001), ICU admission due to medical reason (OR, 3.479; 95% CI, 3.129 to 3.868; p<0.001), admission via emergency room (OR, 2.112; 95% CI, 1.895 to 2.353; p<0.001), others such as the patient admitted the ICU from the cardiovascular room, angiography room, or injection room (OR, 2.274; 95% CI, 1.566 to 3.303; p<0.001), chronic liver disease (OR, 1.515; 95% CI, 1.142 to 2.011; p=0.004), chronic kidney disease (OR, 1.338; 95% CI, 1.063 to 1.684; p=0.013), use of invasive mechanical ventilation (OR, 5.862; 95% CI, 5.194 to 6.616; p<0.001), vasopressors (OR, 2.922; 95% CI, 2.623 to 3.255, and p<0.001); ICU readmission (OR, 1.734; 95% CI, 1.533 to 1.962; p<0.001) (Table 3). In addition, age, male, ICU admission due to medical reasons, admission source, chronic liver disease, transplantation, use of mechanical ventilation, and administration of vasopressors were identified as factors associated with ICU mortality based on logistic analysis (Supplementary Table S5).
Discussion
Our study of 32,322 ICU admissions identified significant changes in the demographics of older ICU patients. Specifically, the average age of these patients increased from 71.9±5.6 years in 2007 to 73.2±6.1 years in 2017. Along with this trend, the percentage of admissions for VVO group (85 years and older) increased from 3.3% in 2007 to 5.0% in 2017. As patients aged, the likelihood of being admitted for medical reasons and female patients increased, while the likelihood of being admitted for surgical reasons and male patients decreased. This trend is consistent with other research. For example, a Korean study observed a rise in the proportion of female ICU patients from 39.3% in 2003 to 42.5% in 2013 [18]. Similarly, Garland et al. [19], found that women admitted to the ICU were older than men (mean 66.1 years vs. 63.5 years). Further, studies by Ihra et al. [20] and Haas et al. [21] have shown a shift toward more older, female patients in the ICU, primarily for medical reasons. The trend is similar across the board, with a French study conducted between 2006 and 2015 showing an increase in the percentage of females aged 90 and older admitted to intensive care units with acute respiratory infections compared to males [22]. In light of these findings, ICUs should prepare for an increasing number of female patients by considering the subtle interplay of gender and age in patient outcomes. A national study [23] found that while male patients generally have higher in-hospital mortality rates, women have higher mortality rates in certain age groups between 19 and 50 years, suggesting that gender-specific health risks exist with age, such as men being more susceptible to respiratory infections and women to urinary tract infections. In an aging society, these patterns indicate the need for health policies to adapt to and address the differential prevalence of conditions such as respiratory, gastrointestinal, and hepatobiliary diseases that affect older patients differently by gender. The findings also suggest that a gender-specific approach to ICU patient management should be adopted to ensure that both male and female patients receive care tailored to their specific health risks and response to treatment [24].
In our study, there was a trend toward higher ICU and hospital mortality rates and longer ICU and hospital LOS, particularly in the VVO group. However, from 2007 to 2017, the overall mortality and ICU and hospital LOS in all older patients tended to decrease. This decline in mortality and LOS can be attributed to a variety of factors [25,26]. Advances in medical technology [27] and treatments [28], more effective management of chronic conditions [29], and improved ICU protocols [30] may have played a role. Increased attention to early rehabilitation [31,32] and efficient discharge planning, as well as the integration of palliative care [33] in the ICU setting, may also have contributed to these positive outcomes. Despite these advancements and general trends, it’s important to note that ICU mortality and in-hospital mortality rates remain disproportionately higher in the VVO group. In this group, both ICU and hospital LOS are longer compared to younger patient cohorts. This finding aligns with broader observations [34,35] that older ICU patients, particularly those in advanced age groups, tend to have higher hospital mortality rates compared to their younger patients. These differences highlight the need for continued efforts to tailor care and protocols to meet the specific needs of the oldest ICU patients to ensure that the benefits of medical advances are equitably distributed across all age groups.
In the VVO group, noninvasive ventilation was more frequently used than in the O or VO groups. This trend likely reflects Korean cultural attitudes favoring the avoidance of invasive treatments for older patients [36,37]. These observations are consistent with the findings of several other studies that have reported similar treatment choice patterns for older patients in other cultural contexts [10,38,39].
In this study, the association between age and hospital and ICU mortality was only significant in the VVO group of 85 years and older. This finding is consistent with recent studies that highlight the vulnerability of the oldest ICU patients. For example, Reinikainen et al. [40] observed a trend of increasing ICU and hospital mortality with increasing age. Similarly, Boumendil et al. [41] reported that patients aged 80 and older were at a higher risk of hospital mortality compared to younger patients, with a significantly higher OR of 1.52. This notion is further supported by data from the Dutch National Intensive Care Evaluation (NICE) registry [7], which showed a fourfold increase in in-hospital mortality for patients aged 85 years and older compared to patients under 65 years. These findings are consistent with other studies [42,43] that have shown poor prognosis for older ICU patients, especially those aged 80 or 85 years and older. Studies [7,44] of prognostic factors in these very old patients have shown that factors such as acute hospitalization, comorbidity, and functional status have a significant impact on survival outcomes. Guidet et al. [45] highlighted that clinical frailty scales can predict 1-month survival after ICU admission in patients over 80 years old. Similarly, Flaatten et al. [44] identified acute hospitalization, progressive age increase, and frailty as key determinants of survival in this demographic. In contrast to this study, some studies [46] have found that in-hospital mortality rates may vary by ICU bed capacity and admission policies, but no significant differences in long-term survival were found by age. In one systematic review [47], age was not a significant factor in ICU mortality but was associated with 6- and/or 12-month mortality.
This study has several limitations. First, because this study was conducted at a single center, it may not be representative of all ICU patients in Korea. However, as a study that analyzed a significant number of older patients, we believe it can reflect the characteristics of actual patients to some extent. Second, if a person was hospitalized multiple times, we used the first hospitalization to exclude them from the analysis. In this process, we may have missed hospitalizations for more serious illnesses. Third, there is a possibility of selection bias because we did not collect data on patients who were not admitted to the ICU, so we could not compare older patients who were admitted to the ICU with those who declined admission. Fourth, we did not have medical records of patients’ functional status prior to hospitalization, which is known to be an important risk factor for prognosis in older adults. Fifth, the patient population in our study did not distinguish between elective and acute surgical cases. A previous study of patients aged 80 and older found higher mortality rates after acute surgery [48]. Although we were unable to distinguish these specific factors based on medical records, we analyzed our data by categorizing hospitalizations according to emergency department, general ward, and other locations. We believe this approach may help us better understand the potential impact.
In conclusion, our study shows that the demographics of the older population in ICUs are changing, with a steady increase in older patients, particularly those aged 75 years and older. The overall mortality rate for older ICU patients decreased, and the analysis suggests that age, particularly up to 84 years, may not be as much of an independent risk factor for ICU mortality as previously thought. The increasing number of female patients and patients with medical conditions require a reassessment of treatment strategies in the ICU. This trend indicates that customized arrangements may be needed, including expanding medical ICU beds, specialized training for healthcare providers in the management of medical conditions, and adjusting equipment and staffing to better meet the needs of patients. Moreover, while the focus here is on female patients and patients with medical conditions, similar considerations may be needed for male patients and other demographics. These findings indicate that ICUs must adapt to evolving demographic trends to ensure an equitable and effective response to the diverse needs of an aging population.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Data Sharing Statement
Data Sharing Statement Full text via DOI
Full text via DOI Supplement1
Supplement1 Print
Print Download Citation
Download Citation






