


Introduction
Surgical resection is the treatment of choice for early stage non-small cell lung cancer (NSCLC). The surgical outcome of these patients is associated with postoperative recurrence. The reported 5-year postoperative recurrence rates of patients with stage I and II NSCLC are approximately 15%-20% and 30%-40%, respectively1,2. It is impossible to predict which patients are at an increased risk of recurrence after surgical resection based on pathological stage alone. Several studies have shown that the risk factors associated with postoperative recurrence include adenocarcinoma (ADC) histology, the serum carcinoembryonic antigen (CEA) level, tumor differentiation, visceral pleural invasion (VPI), and vessel invasion1,3,4. In addition, novel predictors of lung cancer, such as the status of epidermal growth factor receptor (EGFR), KRAS mutation and maximal standardized uptake values (SUVs) of tumors on positron emission tomography (PET) were also associated with postoperative outcomes5,6,7. These results show variety depending on the patient selection or sample size. Another study reported that the risk factors of recurrence were differed between patients with stage I and stage II disease1.
Currently, the definition of high-risk recurrence is poorly established, and the identification of groups who might benefit from more aggressive adjuvant therapy remains a challenge. An accurate assessment of predictors associated with recurrence is helpful to guide effective adjuvant therapy. Therefore, the aim of this study was to investigate the predictors of recurrence in patients with resected early stage (stage I and II) NSCLC. The patterns of tumor recurrence were also analyzed to identify the risk factors associated with locoregional or distant recurrence.
Materials and Methods
1. Study design and patients
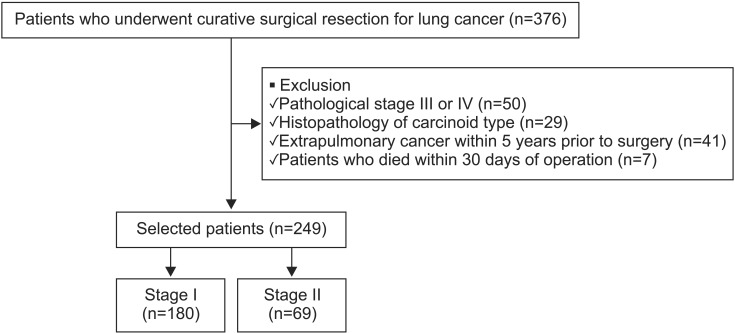
This retrospective study was conducted at the Pusan National University Hospital, Busan, Korea, a university-affiliated tertiary care hospital. We collected the data of 376 patients who underwent curative surgical resection for lung cancer from January 2006 to December 2011. Staging was based on the seventh edition of the American Joint Committee on Cancer (AJCC) TNM staging system. Of these 376 patients, 127 were excluded because of pathological stage III or IV disease (n=50), carcinoid type (n=29), extrapulmonary cancer (n=41), and death within 30 days of operation (n=7). The remaining 249 patients were included in our study (Figure 1). This study was conducted with approval from the Institutional Review Board (IRB) of the Pusan National University Hospital (E-2014154). This study had no impact on patient treatment.
2. Data collection
We reviewed the preoperative clinical data from the medical records of each patient, including the following: age, gender, smoking history, performance status, the serum CEA level, PET SUV of the primary lesion, tumor location and groundglass opacity (GGO) on chest computed tomography (CT). We also reviewed the following postoperative factors: type of resection, pathological TNM stage, histopathology, the grade of differentiation, VPI, lymphovascular invasion (LVI), the surgical margin status, and the status of EGFR and KRAS mutations. The histopathology of patients included ADC, squamous cell carcinoma (SCC), adenosquamous, and others. For analysis, the patients were divided into two groups based on their histology: ADC or non-ADC. Additionally, we collected data concerning the subtypes of ADC that were addressed by the International Association for the Study of Lung Cancer (IASLC), the American Thoracic Society (ATS), and the European Respiratory Society (ERS) in 2011, including adenocarcinoma in situ (AIS), minimally invasive adenocarcinoma (MIA), and invasive ADC8.
Tumor recurrence was determined using clinical assessment, radiographic reports, and/or data from a biopsies. Recurrence within the lymph nodes was defined when a new or enlarging lymph node was more than 1 cm on the short axis on a follow-up CT scan. For patients who underwent PET at the time of disease recurrence, all sites of abnormal uptake that correlated with a lymph node or soft tissue mass were scored. Additionally, pathology confirmation was performed using endobronchial ultrasound-guided transbronchial needle aspiration or endoscopic ultrasound guided fine needle aspiration. The date of recurrence was defined as the date of first detected recurrence. Locoregional recurrence was defined as recurrence in an ipsilateral lobe of the lung, bronchial stump, or a regional lymph node (subcarinal, periesophageal, ipsilateral or contralateral mediastinum, supraclavicular, or hilar lymph nodes)9. Distant recurrence was defined as that occurring in the liver, contralateral lung, adrenal glands, brain, bone, or other location. Simultaneous locoregional and distant recurrence was defined as distant recurrence.
3. Statistical analysis
The continuous data of the entire study population were expressed as medians (25%-75% interquartile range [IQR]), and categorical variables were expressed as numbers (percentages). Student's t test was used to compare continuous variables and the chi-squared test and Fisher's exact test (for small numbers) were used to compare categorical variables. Receiver-operating-characteristic (ROC) curves were constructed to determine cut-off values. The Kaplan-Meier method with the log-rank test was developed to represent the unadjusted factors associated with 5-year recurrence. Variables that had a p-value less than 0.1 were included in multivariate models. Multivariate Cox proportional hazard models were used to identify factors associated with 5-year recurrence, locoregional recurrence, and distant metastasis, which were considered significant at p<0.05. Statistical analyses were performed using the SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA).
Results
1. Clinical characteristics of the study population
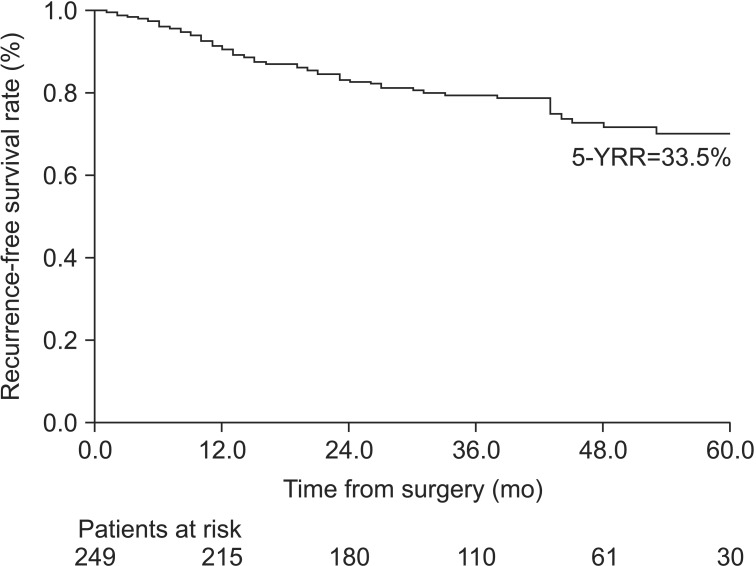
Two hundred and forty-nine patients were included in our study. Among them, 180 patients were stage I, and 69 were stage II. Recurrence during the follow-up was detected in 57 of 249 patients (23.7%). The cumulative risk of recurrence is presented in Figure 2. The median duration of follow-up was 36.5 months (IQR, 28.0-52.8). Median time to recurrence in 57 recurrent patients was 15 months (IQR, 9-27). In most cases (41 of 57, 71.9%), recurrence occurred within 2 years after surgery; in only one case (1.8%), it was found after 5 years following surgery. The most common sites of recurrence were the lung (43.9%) and lymph nodes (40.4%) in all patients. The demographics of all patients and comparison of clinical factors between the patients with or without recurrence during the follow-up are shown in Table 1. Surgical margins were positive in 5.2% (n=13). Among these patients with residual disease, two received postoperative radiotherapy. The number of ADC patients was 158 (63.5%). Among them, the proportions of AIS, MIA, and invasive ADC were 7.7%, 6.3%, and 86.0%, respectively. GGO on CT scan was shown in 20.9% (n=52) of the total patients. Compared with the no-recurrence group, recurrence group had a higher rate of PET SUV >4.5, stage II disease, involvement of the N1 lymph node, presence of VPI, a positive resection margin, the presence of LVI, moderate-poorly differentiated carcinoma, KRAS mutation, and adjuvant chemotherapy. The cut-off values of CEA and PET SUV were determined by the ROC curves for the categorical analysis (data not shown).
2. Risk factors associated with total, local, and distant recurrence
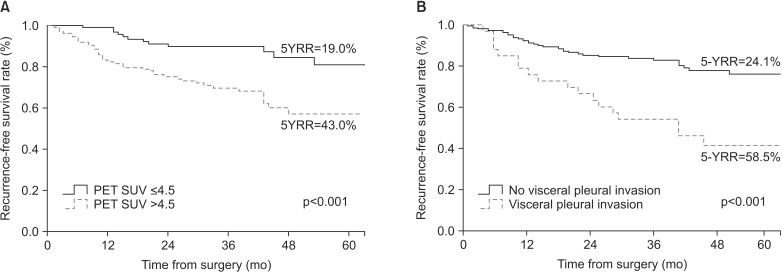
To identify the factors associated with 5-year recurrence in the entire study population, the Kaplan-Meier method with log-rank test and Cox proportional hazard analyses were performed. Nine clinical factors were associated with 5-year recurrence in univariate analysis (p<0.1): stage II disease (p<0.001), involvement of the N1 lymph node (p=0.003), PET SUV >4.5 (p<0.001), VPI (p<0.001), a positive resection margin (p=0.010), LVI (p=0.016), KRAS mutation (p=0.042), moderate-poorly differentiated carcinoma (p=0.005), and adjuvant chemotherapy (p=0.001). In multivariate analysis, PET SUV >4.5 and VPI were independent factors associated with 5-year recurrence (Table 2). Figure 3 shows the Kaplan-Meier survival curves of factors associated with 5-year total recurrence.
Twenty-four patients of the total 249 patients (9.6%) had locoregional recurrence, and 33 (13.3%) had distant recurrence. Factors associated with locoregional recurrence in univariate analysis (p<0.1) included stage II disease (p=0.008), involvement of the N1 lymph node (p<0.001), PET SUV >4.5 (p=0.008), VPI (p=0.010), LVI (p=0.012), KRAS mutation (p=0.015), moderate-poor differentiation (p=0.034), and adjuvant chemotherapy (p<0.001). In multivariate analysis, VPI and involvement of the N1 lymph node were significantly associated with locoregional recurrence (Table 3). In the distant recurrence group, univariate analysis revealed that recurrence was correlated with stage II disease (p=0.008), PET SUV >4.5 (p=0.004), VPI (p<0.001), a positive resection margin (p=0.008), moderate-poorly differentiated carcinoma (p=0.038), and adjuvant chemotherapy (p<0.092). Only VPI was independently associated with distant recurrence in multivariate analysis (p=0.001) (Table 3).
3. Subgroup analysis according to stage
The 5-year recurrence rates for patients with stage I and II NSCLC were 22.9% and 43.5%, respectively (p<0.001). In stage I patients, factors associated with 5-year recurrence were male gender (p=0.052), PET SUV >4.5 (p=0.001), VPI (p<0.001), a positive resection margin (p<0.001), and moderate-poorly differentiated carcinoma (p=0.008) in univariate analysis. In multivariate analysis, male gender, VPI, and a positive resection margin were independently associated with 5-year recurrence (Table 4). In stage II patients, univariate analysis revealed that ADC histology (p=0.023) and EGFR mutation (p=0.095) were significantly associated with recurrence. No clinical factor was significantly associated with recurrence in stage II patients by multivariate analysis.
Discussion
This study investigated the significance of clinical factors other than TNM stage on the time to NSCLC recurrence after complete surgical resection. The presence of VPI and high level of PET SUV of the primary lesion were independent factors associated with postoperative recurrence in early-stage NSCLC patients.
VPI has been mentioned frequently in the various studies concerning the prediction of postoperative recurrence. However, its predictive power has only been confirmed by univariate analysis or appeared to be influenced by the tumor size3,10. In our study, after adjusting for other confounders, VPI was proven to be an independent predictor of recurrence. VPI is defined as invasion to the surface of the visceral pleura or invasion beyond the elastic layer11. The degree of VPI was classified into p0-p2 stages, according to the degree of pleural invasion12. The association of VPI and tumor recurrence has been explained as initial exfoliation in the pleural cavity, followed by preformed stomas that connect the subpleural lymphatics with the pleural space, accounting for the systemic tumor cell dissemination13,14. As these malignant cells spread through the mediastinal lymphatic vessels, the more frequent incidence of N2 disease is observed in VPI14. Thus, N2 disease was excluded in our study, and N1 stage was included as a confounding factor in multivariate analysis. The presence of the VPI allows classification of the primary tumor as T2 when it is 3 cm or less in size, according to the seventh edition of the TNM staging system15. However, recently, some reports have recommended upstaging even if the size of tumor is larger than 3 cm16,17. It may be inferred from these data that VPI is an important predictor of recurrence and prognosis in earlystage NSCLC, independent of the tumor size. Therefore, adjuvant therapy should be more likely to be recommended in patients with VPI.
Although PET SUV has not been clearly identified in association with the recurrence of cancer, several studies have reported that SUV is a prognostic factor for recurrence 7,18,19. This may be because the more metabolically active is the tumor, the worse the outcome will be. However, each of the studies reported different SUV cut-off values20,21. The SUV values were determined by plasma glucose levels, tumor size, and type of neoplasm7,22. In particular, regarding the relationship between SUV and the tumor histopathology, a previous study showed that the SUV was significantly higher in SCC than ADC19,23. In our study, the cut-off SUV value of 4.5 was determined by the ROC of all patients, and the same cut-off value was applied to both ADC and SCC. We performed subgroup analysis, which applied different cut-off values of SUV according to the histologic subtypes. The median value of SUV was significantly different between these groups (p<0.001): ADC, 3.6 (IQR, 2.1-6.5); SCC, 9.9 (IQR, 6.5-12.5). In the ADC group (n=158), a PET SUV ≥2 was significantly associated with 5-year recurrence by the Kaplan-Meier with log-rank test. No one has shown recurrence in patients with SUV <2. In addition, the proportion of GGO in the total patients was 20.9%. The result was not changed after excluding the patients with GGO. However, in the SCC group, there was no significant association between a high level of PET SUV and tumor recurrence with a cut-off value of 9 or 10. This suggests that PET SUV may play an important role in the outcomes of ADC patients, but not in those of SCC patients. However, studies concerning the relationship between PET SUV and the recurrence of earlystage NSCLC, particularly ADC patients, are rare. Thus, further study is needed to confirm our findings.
In the analysis of stage I patients, VPI and positive margin status were independent risk factors of recurrence. However, in stage II patients, only ADC was associated with recurrence by univariate analysis. These results were similar to a previous study that found the risk factors differed between patients with stages I and II disease1. In patients with AIS or MIA, disease-specific survival was almost 100% after complete resection. However, invasive ADC, particularly micropapillary or solid-predominant, has a more aggressive behavior that favors early distant metastasis24. In our study, the proportion of GGO was significantly high in stage I (38.1%) compared with that in stage II patients (6.3%) (p<0.001). Additionally, AIS or MIA were included among stage I, but not among stage II patients. Among patients with invasive ADC, the proportion of micropapillary or solid-predominant subtypes was higher in stage II (28.0%) than in stage I patients (12.8%) (with no statistical significance). These results indicate that more aggressive subtypes would be included in stage II than in stage I disease. Therefore, ADC could be a poor prognostic factor in stage II, but not stage I, disease, instead of other factors, such as VPI, which played a more important role in recurrence for stage I patients.
We also analyzed the patterns of recurrence and factors associated with locoregional or distant recurrence. Although there is variation in the literature, it is generally believed that the risk of local recurrence for patients with early-stage NSCLC is low9,25. Several studies have explained the finding as follows. First, local recurrence may be missed because it is difficult to detect from an isolated lymph node or stump site recurrence9. In addition, concurrent local and distant recurrences are common, and they are regarded as distant recurrences. However, it is possible that local recurrence occurred before and may not be detected until distant recurrence developed. Another explanation is that the definition of local failure varies widely. Some studies defined local failure as occurring only in the ipsilateral lung and mediastinum9. However, the contralateral lymph nodes were classified as local failure in other studies26. Our study showed that the frequency of distant recurrence appeared to be similar to that of local recurrence. This is because the most common recurrence site was the lymph nodes and contralateral mediastinal recurrence was regarded as local failure.
Previous studies reported that clinical factors associated with local or distant recurrence were different from each other3,26. Factors associated with local recurrence included diabetes and LVI. On the other hand, distant recurrence was associated with histology type, such as ADC, performance of pneumonectomy, and advanced stage in other studies26. However, evidence to confirm these findings is lacking. In our study, only VPI was shown to be associated with both local and distant recurrence. Involvement of the N1 lymph nodes was an independent risk factor of locoregional recurrence. Because the number of patients with recurrence was small and the duration of the follow-up was short, the interpretation of these results should be limited. Information from larger population studies is warranted to determine the factors associated with the patterns of recurrence in early-stage NSCLC.
There were several limitations to this study. First, its retrospective nature resulted in various biases, and study was performed at a single center. Thus, the patient characteristics may not be representative. Second, because the follow-up duration was insufficient, we could not perform an analysis of the overall survival rate of patients. Third, the rate of a positive resection margin was higher (5.2%) compared with that in previous studies3,9, and postoperative radiotherapy or re-surgery was only performed to two patients.
Another limitation of our study is that recurrence group had a higher rate of receiving adjuvant chemotherapy compared with no-recurrence group (Table 1), and adjuvant chemotherapy was associated with 5-year recurrence in multivariate analysis (with no statistical significance) (Table 2). When we analyzed the clinical characteristics of patients receiving adjuvant chemotherapy compared with non-receiving patients in stage I disease, they had a higher rate of a positive margin, mod-poorly differentiated carcinoma, and KRAS mutation. These factors are more likely to influence tumor recurrence, and suggest that patients with a high risk of recurrence are likely to have received adjuvant chemotherapy in stage I disease. In addition, adjuvant chemotherapy is standard therapy in stage II disease; however, only 47.8% of stage II patients in our study received adjuvant chemotherapy. Therefore, this must be considered in the interpretation of the results. Despite these limitations, our study presented current issues regarding predictors of recurrence after curative resection and which patients will benefit from adjuvant therapy.
In summary, our study shows that the presence of the VPI and a preoperative high level of PET SUV were independent factors associated with postoperative recurrence in earlystage NSCLC patients. Although the risk factors associated with recurrence would differ between stage I and II, patients with these risk factors should be considered for more aggressive adjuvant therapy. Prospective, large-scale multicenter studies with longer follow-up periods are required to identify the predictors of postoperative outcomes.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






