



Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of mortality and morbidity with a high economic and social burden globally [1]. Small airways are the major sites of pathology in many respiratory diseases, including COPD [2]. The airways distal to the 8th generation are small airways with an internal diameter <2 mm. Small airways include a portion of conducting airways and gas-exchanging areas [2]. Small airway dysfunction (SAD) is considered a precursor for the development of emphysema [3]. Mucous hypersecretion, mucous plugging of the small airways, and immune cell infiltration are the pathophysiological mechanisms of SAD in COPD [3].
There are no standard criteria for diagnosing SAD [4]. Large airways substantially contribute to forced expiratory volume 1 second (FEV1) [5]. Therefore, FEV1 is not specific to SAD. Maximal mid-expiratory flow (MMEF) <65% predicted is considered a predictor of SAD in spirometry [4]. However, MMEF has poor reproducibility and high variability in detecting SAD [2,5]. Respiratory impedance measured by the forced oscillation technique and impulse oscillometry is an easy, effort-independent, and noninvasive technique for diagnosing SAD [5]. Impedance parameters such as respiratory system reactance at 5 Hz (X5), the difference in whole-breath resistance at 5 and 20 Hz (R5-20), resonant frequency, and the area under the reactance curve between 5 Hz and resonant frequency are used to diagnose SAD [4]. The prevalence of SAD in patients with COPD and its association with clinical parameters and the effects of treatment, especially in the Indian population, has not been explored.
The primary objective of this study was to estimate the prevalence of SAD in stable COPD patients using oscillometry and to determine its association with lung function, COPD assessment test (CAT) scores, and a 6-minute walk test (6MWT). The secondary objective was to assess changes in impedance, lung function, and symptom burden after 3 months of Global Initiative for Chronic Obstructive Lung Disease (GOLD) guided treatment.
Materials and Methods
1. Study design and population
We prospectively screened consecutive patients aged >40 years from the outpatient department between August 2021 and January 2023. The diagnosis of COPD was made according to the GOLD guidelines with a ratio of post-bronchodilator (post-BD) FEV1 and forced vital capacity (FVC) <0.70. The exclusion criteria were a history of acute COPD exacerbation or hospitalization within 4 weeks before recruitment, structural lung diseases, including active or previous tuberculosis, bronchiectasis, and moderate to severe coronavirus disease 2019 (COVID-19) in the past 12 months.
The Institutional Ethics Committee, All India Institute of Medical Sciences, Raipur (India) approved the study protocol (No: 1863/IEC-AIIMSRPR/2021 date 21/08/2021). Written informed consent was obtained from all participants. This study was conducted in accordance with good clinical practices and the Declaration of Helsinki.
2. Assessments
At the baseline visit, demographic information, including sex, age, height, weight, smoking history, medication history, comorbidities, and the number of previous COPD exacerbations, was collected. The impact of COPD symptoms on health status was assessed using CAT scores (Hindi translation). Based on the history of previous exacerbations and CAT scores, the severity of COPD was graded as per the GOLD guidelines [1].
3. Forced oscillation technique
The respiratory system resistance and reactance were measured at 5, 11, and 19 Hz, respectively, using a Resmon Pro Full device (RestechSrl, Milan, Italy) as per the recommendations of the European Respiratory Society [6]. At least three tests were performed, and each continued until ten accepted breaths were recorded. The mean of three trials was used for analysis only if the coefficient of variation for R5 was <10%. The evaluated parameters were whole- and within-breath respiratory system resistance at 5 Hz (R5) and X5, the difference in inspiratory and expiratory reactance at 5 Hz (∆X5), and the difference in whole-breath resistance at 5 and 19 Hz (R5-19). The regression equations of oscillometry for the Indian population were used to define the upper limit of normal (ULN) and lower limit of normal (LLN) [7]. SAD was defined as R5-19 >ULN or X5 <LLN. The expiratory flow limitation at tidal breath (EFLT) was defined as ∆X5 ≥0.28 kPa/L/sec [8].
4. Spirometry
After oscillometry, the patient underwent spirometry, including body plethysmography and single-breath CO diffusion capacity, using PowerCube Body+ (GANSHORN Medizin Electronic, Niederlauer, Germany) as per the American Thoracic Society/European Respiratory Society recommendations [9]. Predictive equations of the spirometry parameters for the Indian population were used [10]. In our study, an MMEF <65% of predicted is considered to be a spirometry-defined SAD. The diffusing capacity of the lungs for carbon monoxide (DLCOc) was adjusted for hemoglobin. The Global Lung Initiative 2012 predictive equations for lung volumes and DLCOc were used [11].
Both lung function tests and oscillometry were repeated 15 minutes after 400 μg salbutamol inhalation from a metered-dose inhaler with a spacer device. Post-BD reversibility in spirometry was defined as a ≥12% increase from the pre-BD value and a ≥0.2 L increase in either FEV1 or FVC. As per the GOLD guidelines, the severity of airflow obstruction was classified on the basis of post-BD FEV1% of the predicted value [1]. The bronchodilator responsiveness of R5 was defined as a (-)40% decrease and a (+)50% increase in X5 from the pre-BD value [5].
A 6MWT was performed on an undisturbed 30-m hospital corridor according to standard guidelines [12]. We measured the 6-minute walk distance (6MWD), desaturation after the test, and the change in dyspnea score using the Borg score. All investigations as mentioned above were repeated during follow-up visits at 3 to 6 months.
5. Statistical analysis
The data were analyzed using IBM SPSS statistics for Windows version 23.0 (IBM Corp., Armonk, NY, USA). Data are presented as the standard deviation for continuous variables and frequency (percentage) or median (interquartile range [IQR]) for nominal variables. Unpaired and paired t-tests, Pearson χ2 tests, and analysis of variance (ANOVA) with post hoc tests were used for comparisons where appropriate. Relationships across parameters were examined using Pearson’s correlation coefficient (r). A value of p<0.05 was considered statistically significant.
Results
1. Patient characteristics
We recruited 330 patients, of whom 196 were eligible for the study. The details of the study population enrollment are shown in Figure 1. Our study cohort was mostly male (95.9%), and the mean age was 63.3 years. The demographic and clinical profiles of the study population are summarized in Table 1. Nearly half of the study population was treatment naïve (n=100, 51%). The majority was either current or ex-smokers (86.7%). The median pack-years of smoking were 32.9 pack-years. According to the GOLD taxonomy, the distributions of COPD-C, COPD-P, and COPD-U were 80.1%, 14.3%, and 5.6%, respectively. Most patients were in GOLD group B (54.6%), followed by group E (26.5%). The median peripheral blood eosinophil count was 120/mm3 (IQR, 30 to 230). The most common comorbid was systemic hypertension (32.1%), followed by diabetes mellitus (24.5%).
2. Forced oscillation technique
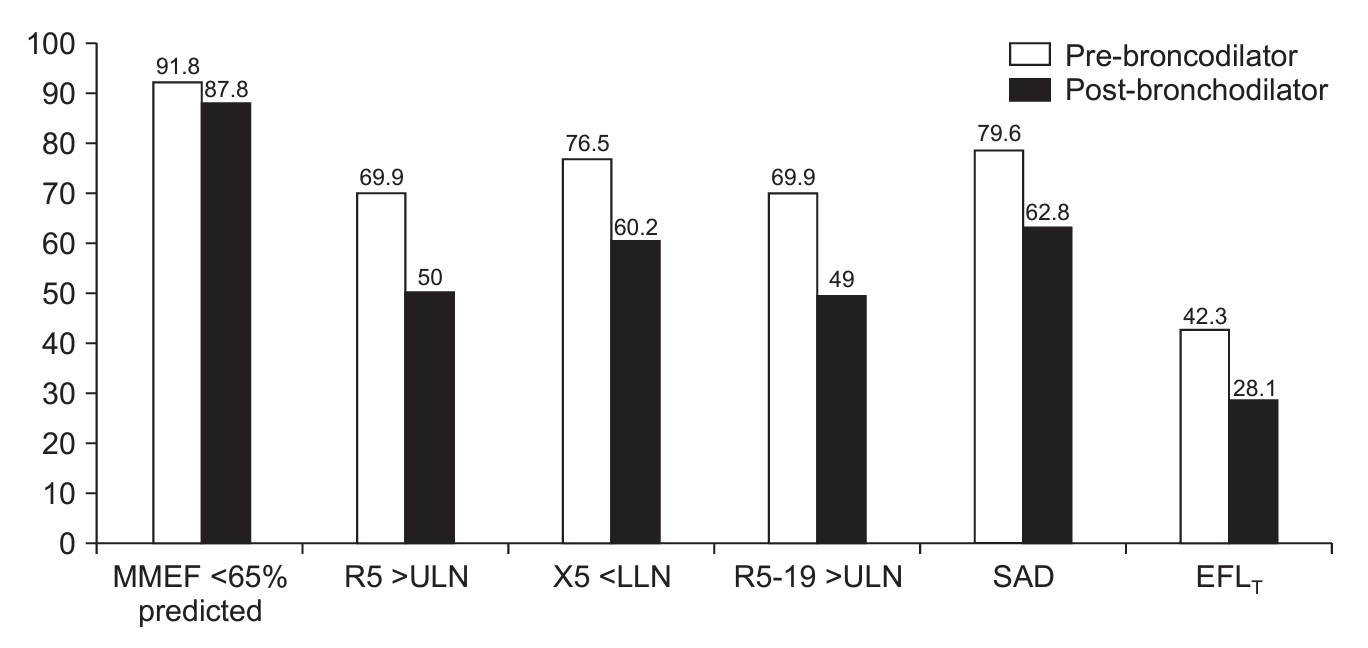
The coefficient of variation of the R5 measurements was 5.37%±2.59%. Post-BD normal R5 (≤ULN), X5 (≥LLN), and R5-19 (≤ULN) were observed in 50%, 39.8%, and 51% of the patients, respectively. Pre-BD SAD was observed in 79.6% of the patients, which was reduced to 62.8% (95% confidence interval [CI], 56.1 to 69.9) after post-BD (Figure 2). The prevalence of preBD EFLT was 42.3%, but it was reduced to 28.1% (95% CI, 21.9 to 34.2) in post-BD. The prevalence of SAD was similar in both treatment-naive and those already on-treatment for COPD (50.4% vs. 49.6%, p>0.05). The bronchodilator responsiveness of R5 and X5 was 11.2% and 15.8%, respectively. A paradoxical bronchodilator response in X5 (i.e., >50% increase) was observed in 2.5% of the cohort. Large airway dysfunction, i.e., postBD R19 >ULN, was observed in 38.5% of the patients. Isolated large airway dysfunction without underlying SAD was observed in 8.7% of the patients.
3. Baseline lung function parameters
The mean post-BD FEV1% predicted of the cohort was 56.4% (Table 1). Bronchodilator responsiveness in FEV1 and FVC was observed in 26.5% and 42.3%, respectively. According to the GOLD classification, the majority of the patients had grade 2 (44.9%), followed by grade 3 (33.2%) airflow obstruction. The mean MMEF of the cohort was 38.3% of the predicted. Spirometry-defined SAD was observed in 87.8% of the patients. The mean total lung capacity (TLC) was 5.6 L. The median DLCOc was 65% of that predicted.
4. COPD severity
The age of the patients was not different across the GOLD grades (Table 1). Post hoc analysis CAT scores were not significantly different among GOLD grades 2-4. The severity of air trapping (ratio of residual volume to TLC [RV/TLC], % of predicted) and impairment in DLCOc increased with the severity of GOLD grading. Higher GOLD grading was significantly associated with respiratory impedance abnormalities, including SAD. The prevalence of EFLT also significantly increased with higher GOLD grades. Post hoc analysis showed that R5 and R19 were not different between GOLD grades 3 and 4. Reduced 6MWD, increased desaturation, and dyspnea during 6MWT were observed in patients with higher COPD grades. The prevalence of spirometry-defined SAD was significantly higher than that of oscillometer-defined SAD, irrespective of the severity of COPD (87.8% vs. 62.8%, p<0.01).
The lung function parameters across the GOLD grouping of COPD patients are presented in Table 2. The FEV1% predicted, MMEF% predicted, and DLCOc reduced significantly in the higher GOLD groups. R5, X5, R5-19, and the prevalence of SAD also increased in the higher GOLD groups. The abnormalities in large airways, i.e., R19 >ULN, were not different between GOLD group B and E. The prevalence of EFLT was also not different across the GOLD groups. The COPD patients in the higher GOLD groups had significantly shorter 6MWD (p<0.01).
5. COPD patients with SAD
COPD patients with oscillometry-defined SAD had more severe airflow obstruction (post-BD FEV1% of predicted 46.6% vs. 72.8%, p<0.01), more air trapping (post-BD RV/TLC% of predicted 159.7% vs. 129%, p<0.01), and reduced DLCOc, but had similar TLC (Table 3). COPD patients with SAD had significantly reduced 6MWD, more desaturation, and more breathlessness than those without SAD.
We observed that 44.7% (95% CI, 36.6 to 53.7) of COPD patients with SAD had EFLT. COPD patients with the EFLT phenotype had significantly more severe lung function impairment, including diffusion impairment, than those with SAD and without EFLT (Table 4). COPD patients with EFLT reported more severe breathlessness after a 6MWT. However, the desaturation and distance covered during the 6MWT were not different between the groups. The univariate correlation between the CAT score, lung function, and impedance parameters was low (r<0.3) but significant (p<0.05).
6. Follow-up
Patients received either single or combinations of inhaled long-acting bronchodilators and or inhaled corticosteroids based on GOLD recommendations. A total of 72 patients reported for follow-up. Of these, 59 patients were eligible for follow-up evaluation; the reasons for these exclusions are mentioned in Figure 1. The mean interval between baseline and follow-up visits was 4.1±2.2 months. Except for the improvement in the CAT scores and R5, there were no significant improvements in lung function or impedance parameters (Table 5).
Discussion
This study explored the prevalence of oscillometry-defined SAD in a cohort of stable COPD patients. This study highlights the high prevalence of SAD and EFLT in patients with COPD, particularly in those with severe diseases. The prevalence of oscillometry-defined SAD was significantly lower than that of spirometry-defined SAD across all COPD severities. The presence of SAD in patients with COPD signifies severe lung function impairment and a higher symptom burden.
The involvement of small airways is part of the natural history of COPD. Computed tomography of resected lung samples of patients with COPD demonstrated narrowing of small airways that appear before the onset of emphysema and increase with the disease severity [13].
The GOLD guidelines recommend post-BD spirometry parameters to define the severity of airflow obstruction in patients with COPD [1]. Whether post-BD impedance can be used to assess SAD in COPD remains to be determined [6]. However, to maintain uniformity with the spirometry parameter, we used the post-BD impedance parameters. The bronchodilator response in respiratory impedance (either R5 or X5) was significantly less than that in spirometry (20.4% vs. 49.5%, p<0.01). The bronchodilator response in the spirometry parameters of our cohort was similar to that reported in a previous study [14].
Various investigators have investigated the prevalence of oscillometry-defined SAD in COPD and its impact [15-18]. However, the impedance parameters and cutoff values used to define SAD in these studies were diverse. Using a fixed R5-20 cutoff (>0.03 kPa/L/sec), Pisi et al. [15] observed that 80% of COPD patients (n=100) had SAD. Crisafulli et al. [16] reported a lower prevalence of SAD in COPD patients (n=202) with a higher R5-20 cutoff (≥0.07 kPa/L/sec). Based on the pre-BD R5-19 cutoff ≥0.07 kPa/L/sec, the prevalence of SAD in our study was 82.7%, which is slightly higher than that in previous studies. Crim et al. [17] evaluated respiratory impedance in the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) cohort of COPD patients (n=2,054). They observed beyond normal X5, R20, and R5-20 in 66%, 14%, and 60%, respectively. The prevalance of abnormal X5 in our study was similar, but the R19 ≥ULN was higher. We also observed abnormality in large airways, i.e., R19 was independent of underlying SAD. Recently, Lu et al. [18] used the ULN or LLN of the local population to assess abnormal respiratory impedance in COPD patients (n=768) of the Early Chronic Obstructive Pulmonary Disease (ECOPD) cohort from China. The proportion of impairment in R5, X5, and R5-20 in their study varied from 52.9% to 62.5%, similar to our observations. The prevalence of SAD across studies was variable because of the variable proportion of severe COPD in the cohorts, parameters used to define SAD, cutoff values, and probably different ethnicities.
We observed that the prevalence of SAD progressed with GOLD severity, and all patients with GOLD grade 4 had SAD. Similarly, Lu et al. [18] observed that the abnormality in impedance progressively increased from 25% to 100% in GOLD stages 1 to 4. Crisafulli et al. [16] also reported progressively increasing SAD prevalence with GOLD severity.
Collapsing of the small airways during tidal breath increases the ∆X5. A higher RV/TLC% reduces elastic lung recoil and increases ∆X5 in COPD patients [19]. A threshold value of ∆X5 ≥0.28 kPa/L/sec during tidal breathing has high specificity and sensitivity to diagnose EFLT [8]. Paredi et al. [20] observed that ∆X5 in COPD patients was higher than that in asthma patients, and ∆X5 can differentiate between these two diseases. Beech et al. [21] observed that 47.8% of COPD patients (n=70) had EFLT. Dean et al. [22] found that 37.4% of COPD patients (n=147) had EFLT. The pre-BD EFLT of our cohort was 41.3%, which is comparable to both studies [21,22]. Mikamo et al. [19] examined the effects of EFLT among 74 patients with COPD using a lower cutoff of ∆X5 (0.55 cm H2O/L/sec). All the above studies reported that the presence of EFLT was associated with a significantly higher lung function abnormality, but the effects on symptom scores varied across the studies. Aarli et al. [23] observed that COPD patients (n=425) with ∆X5 ≥ULN were associated with poor exercise performance, more exacerbations, more hospitalizations, and higher mortality. We observed that EFLT was present in a subgroup of COPD patients with SAD and the presence of EFLT was associated with further lung function impairment.
Anderson and Lipworth [24] observed that the severity of dyspnea, measured by the Medical Research Council dyspnea score, had a poor correlation with respiratory impedance and lung function parameters. Crisafulli et al. [16] reported a significant correlation between R5-20 and CAT. The correlation coefficient between impedance parameters and the CAT score in our study was weaker than that in previous studies. In the present study, 6MWD and desaturation during 6MWT showed a significant but weak correlation with lung function and impedance parameters.
Dean et al. [22] reported no significant changes in ∆X5 values in patients with COPD between baseline and after 2 years of treatment, irrespective of baseline EFLT. Beech et al. [21] also observed that despite 6 months of treatment, EFLT persisted in the majority of patients. Crim et al. [17] found little variability in impedance parameters over 3 months. In our study, the prevalence of SAD was similar between treatment-naïve and on-treatment patients, and there was little variability in impedance parameters after 3 months of treatment.
This study had several limitations. It was a cross-sectional study conducted at a single center. Because this was a hospital-based study, severe COPD and symptomatic patients constituted most of the cohort. There were few female patients because smoking is less prevalent among Indian women. Few patients attended follow-up visits. Because an older version of the oscillometry software was used during the study, we could not measure the resonant frequency and the resonant area for all the patients.
The major strength of this study was the use of ULN and LLN of the local population to define abnormalities in respiratory impedance. Post-BD impedance was used to define abnormalities and maintain uniformity with spirometry parameters.
In conclusion, SAD and expiratory flow limitation are present across all COPD severities. The prevalence of SAD increases with increasing GOLD grades. The bronchodilator responsiveness of the impedance parameters in patients with COPD was significantly less than that of the spirometry-defined SAD. The presence of SAD was associated with poor lung function, higher symptom burden, and more desaturation during 6MWT. SAD in patients with COPD remains unaffected despite optimal treatment. A larger cohort and long-term follow-up are necessary to understand the long-term implications of SAD in COPD patients. There is a need to develop a consensus on whether pre- or post-BD impedance parameters should be used to assess oscillometry abnormalities in patients with COPD.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Data Sharing Statement
Data Sharing Statement Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






