



Introduction
Patients with chronic obstructive pulmonary disease (COPD) are at an increased risk developing pneumonia compared with those without COPD. The reported incidence of community-acquired pneumonia (CAP) in hospitalized adult patients with COPD was approximately 10-fold higher than that of the general population in a prospective United States population-based cohort study [1]. Moreover, COPD is reportedly the most commonly observed comorbidity in hospitalized patients with pneumonia [2]. Pneumonia and COPD have similar risk factors for disease development. Cigarette smoking, smoke from biomass fuel, and occupational dust or fume exposure are major risk factors for COPD and also known risk factors for CAP. Poor nutritional status, low income, and limited access to the healthcare system are socioeconomic determinants of both pneumonia and COPD [3]. Mechanistically, pathological changes in COPD, including mucus hypersecretion, diminished mucociliary clearance, disrupted epithelial barrier, and inhibited immune cell migration, could be attributed to the increased risk of pneumonia [4].
Inhaled corticosteroid (ICS) administration is an important treatment option for COPD management. However, ICS therapy is recommended for patients with treatable traits who experience frequent exacerbations and have increased eosinophil counts [5]. In contrast to other bronchodilators, such as long-acting muscarinic antagonist (LAMA) and long-acting ╬▓2 agonist (LABA), ICS could increase the susceptibility to acquiring lower respiratory tract infections [6]. In particular, real-world observational studies of COPD including patients with various comorbidities consistently demonstrated an increased risk of pneumonia with ICS use [7].
Patients of pneumonia with COPD demonstrated poorer outcomes than those without COPD in terms of the severity of pneumonia, frequency of hospitalization, and mortality [8]. However, few studies have evaluated the clinical implications of ICS use in patients with pneumonia. This study aimed to compare the severity and outcomes of pneumonia in patients with COPD with and without prior ICS use.
Materials and Methods
1. Study design and patient identification
We performed a retrospective medical chart review and descriptive analysis of patients with COPD who were admitted to a single tertiary center, Wonju Severance Christian Hospital in Korea during 2019 to 2021 for pneumonia. Study participants were initially selected using corresponding diagnostic codes, such as COPD (J42-J44) and pneumonia (J10-J18), among all the hospitalized patients. The chest radiography or computed tomography findings were reviewed, and pneumonia was confirmed by a radiologist. The exclusion criteria were as follows: (1) no bronchodilator use before occurrence of pneumonia; (2) no radiologically proven pneumonia or misdiagnosis of pneumonia; (3) active treatment for lung cancer, such as radiotherapy or chemotherapy; and (4) incompatibility with the COPD definition upon spirometry even if the patients received bronchodilator treatment for COPD. Patients were classified into ICS and non-ICS users according to the treatment strategy for COPD management prior to the occurrence of pneumonia.
This study was approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR323121). The requirement for informed consent was waived owing to the retrospective nature of the study.
2. Data collection
Patient demographics, including age, sex, comorbidities that could affect the development of pneumonia, spirometry test results, and inhaler type prescribed to patients before pneumonia, were collected from the electronic health records. The spirometry results obtained most recently during stable status before pneumonia were considered for the analysis. Some patients who received treatment for COPD at other hospitals did not have spirometric data before pneumonia onset. In this case, spirometry results after resolution of pneumonia were used for the analysis. Predicted forced expiratory volume in 1 second (FEV1) % was classified according to the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) grade: 1, Ōēź80%; 2, 50%-79%; 3, 30%-49%; 4, <30%. The inhaler type was determined based on the last prescribed inhaler before hospitalization for pneumonia. Exacerbation history before 12 month of pneumonia was assessed. Exacerbation is considered present if patients received treatment with antibiotics and/or oral corticosteroids (moderate), or if patients visited the emergency room or required admission (severe).
Clinical and laboratory findings at the initial presentation at the hospital were collected. Most patients were admitted to the emergency department. Therefore, the clinical and laboratory assessments were performed in the emergency room. Clinical severity of pneumonia was assessed using the CURB-65 score: confusion; uremia (blood urea nitrogen >19 mg/dL); respiratory rate (Ōēź30/minute); hypotension (systolic blood pressure <90 mm Hg or diastolic blood pressure Ōēż60 mm Hg); and age (Ōēź65 years or older) [9]. Radiological severity was assessed using the following criteria: multilobar infiltration (involvement of more than two lobes), pleural effusion, and complicated pneumonia (empyema or pulmonary abscess).
3. Pneumonia outcomes
Defervescence time was defined as the time (days) taken until improvement of the fever (Ōēź37.8┬░C). The presence of drug resistant pathogens, such as methicillin-resistant Staphylococcus aureus, extended-spectrum ╬▓-lactamase-producing Enterobacteriaceae, and other multidrug-resistant bacteria, was determined through sputum culture. Identification was confirmed when administering restricted antibiotics targeted against these pathogens. Mechanical ventilation included invasive or noninvasive mechanical ventilation for the treatment of COPD and pneumonia during admission. Patients with chronic hypercapnia who received noninvasive ventilation for COPD treatment before admission for pneumonia were not considered as receiving mechanical ventilation. The proportion of patients treated for pneumonia in the intensive care unit (ICU) was also identified. The mortality of patients at 30 and 90 days from the first day of presentation to the hospital regardless of the cause of mortality was evaluated.
4. Statistical analysis
Descriptive statistics were performed and are described as mean value┬▒standard deviation for the continuous variables and as percentage of the number of patients for the categorical variables. The baseline clinical characteristics of ICS and non-ICS users were compared using the Mann-Whitney U test or independent t-test for continuous variables and the chi-square test for categorical variables. Multivariate linear regression analyses were used to determine the factors influencing defervescence time and the length of hospital stay. Additionally, multivariate logistic regression analyses were employed to identify the factors associated with mechanical ventilation, ICU care and mortality. Statistical significance was set at p<0.05. All the statistical analyses were performed using SPSS Statistics software version 25.0 (IBM Corp., Armonk, NY, USA).
Results
1. Baseline characteristics
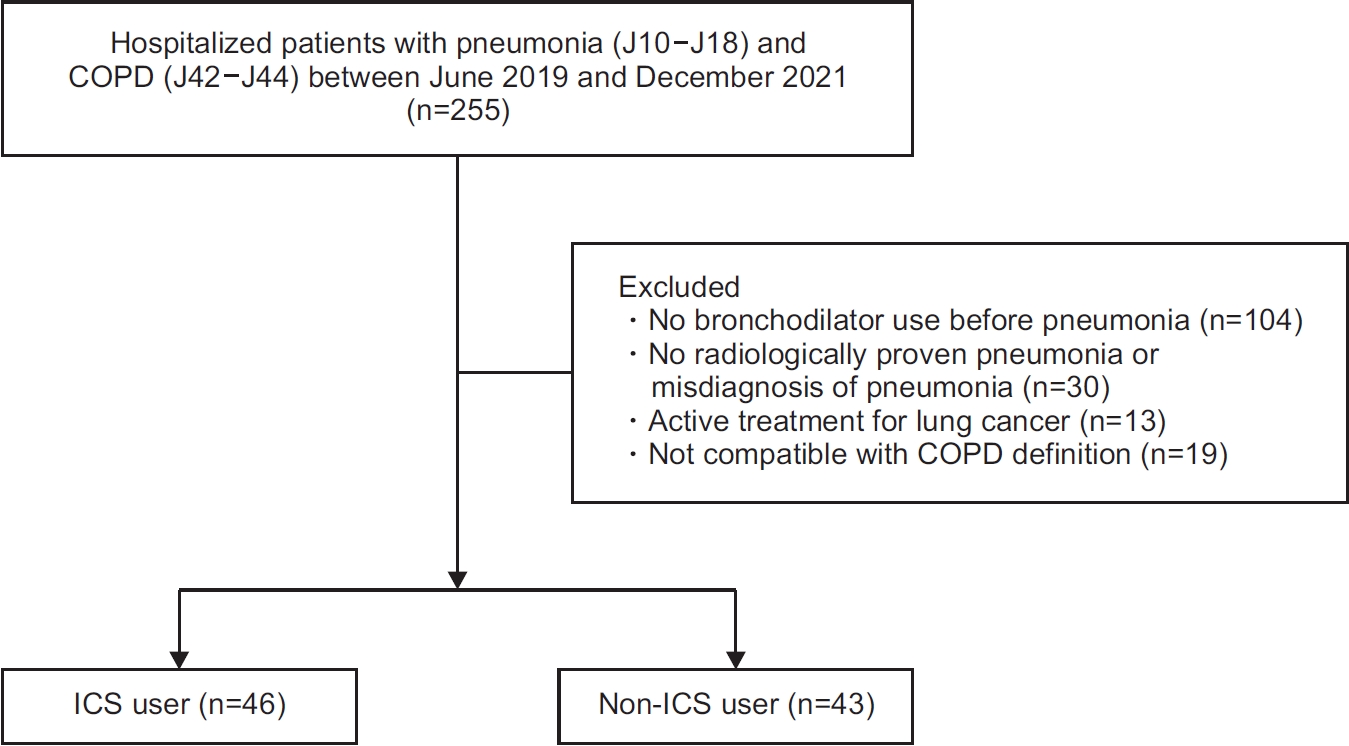
A total of 255 patients with diagnostic codes for both pneumonia and COPD were admitted between June 2019 and December 2021 (Figure 1). Patients who did not have a record of bronchodilator use before admission for pneumonia (n=104), had no radiologically proven pneumonia or misdiagnosis of pneumonia upon reviewing the chest radiographs and computed tomography scans (n=30), were on active treatment for lung cancer (n=13), and demonstrated incompatibility with the COPD definition upon spirometry (n=19) were excluded. The final analysis included 46 ICS users and 43 non-ICS users. Our study period (2019 to 2021) overlapped with the coronavirus disease 2019 (COVID-19) pandemic. Thus, all the patients were screened for COVID-19 before admission. None of the patients were diagnosed with COVID-19.
The mean age of the ICS and non-ICS users was 73.7┬▒9.6 and 75.4┬▒8.4 years, respectively (p=0.381). The proportion of male patients among the ICS and non-ICS users was 93.0% and 89.1%, respectively (p=0.521). The mean FEV1 was 60.4%┬▒21.2% and 59.1%┬▒23.4% for the ICS and non-ICS users, respectively (p=0.785). The distributions of comorbidities and GOLD spirometry grades were comparable between the two groups (Table 1). Among the ICS users, 34 (73.9%) were treated with ICS/LABA/LAMA and 12 (26.1%) with ICS/LABA. The most frequently used ICS was fluticasone propionate (37.0%) and fluticasone furoate (34.8%), followed by budesonide (13.0%), beclomethasone (8.7%), and ciclesonide (6.5%). Among the non-ICS users, 37 (86.0%) were treated with LAMA/ LABA and six (14.0%) with LAMA.
2. Severity of pneumonia
The clinical and laboratory findings at initial presentation were compared between the ICS and non-ICS users (Table 2). The pulse rate was 100.6┬▒23.8 and 98.1┬▒26.7 for the ICS and non-ICS users, respectively (p=0.649). Systolic blood pressure was 136.2┬▒25.4 and 134.8┬▒28.4 for the ICS and non-ICS users, respectively (p=0.807). The diastolic blood pressure, respiratory rate, and body temperature were comparable between the two groups. The leukocyte and C-reactive protein levels were higher in the ICS users, whereas the procalcitonin levels were higher in the non-ICS users. However, the difference was not statistically significant.
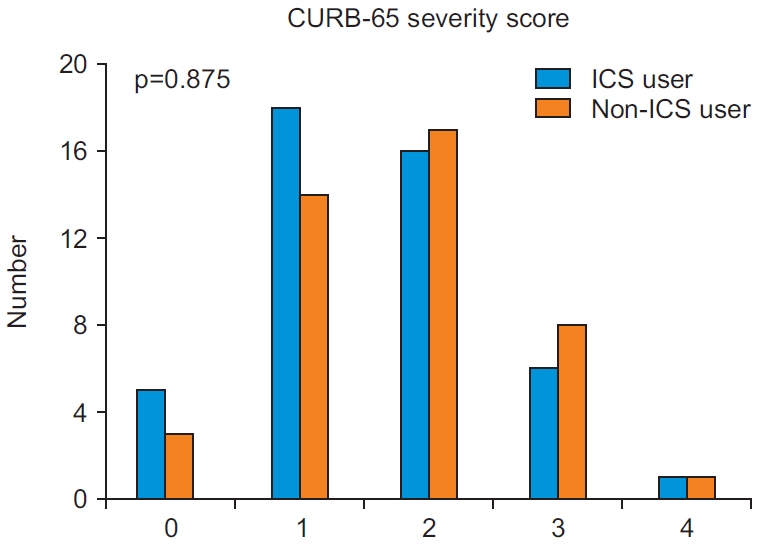
The clinical severity of pneumonia was assessed using the CURB-65 score (Figure 2). Scores of 0, 1, 2, 3, and 4 were reported in five (10.9%), 18 (39.1%), 16 (34.8%), six (13.0%), and one (2.2%) ICS users, respectively. Scores of 0, 1, 2, 3, and 4 were reported in three (7.0%), 14 (32.6%), 17 (39.5%), eight (18.6%), and one (2.3%) non-ICS users, respectively. The distribution of the CURB-65 scores did not differ between both the groups (p=0.875). Radiological severity was also analyzed. Multilobar infiltration and complicated pneumonia were more common in the ICS users, whereas pleural effusion was more common in the non-ICS users. However, no significant factors were identified.
3. Pneumonia outcomes
The defervescence time was 1.5┬▒0.8 and 2.3┬▒2.6 days for the ICS and non-ICS users, respectively (p=0.702) (Table 3). Seven (15.2%) ICS and six (14.0%) non-ICS users received mechanical ventilation (p=0.866). Six (13.0%) ICS users and three (7.0%) non-ICS users received treatment in the ICU (p=0.343). The length of hospital stay was not significantly different between both the groups (13.8┬▒16.4 for ICS users and 11.4┬▒9.2 for non-ICS users, p=0.407). The 30-day mortality rate was 8.7% (four deaths) and 4.7% (two deaths) in the ICS and non-ICS users (p=0.447), respectively, while the 90-day mortality rate was 13.0% (six deaths) and 16.3% (seven deaths) in the ICS and non-ICS users, respectively (p=0.303).
In multivariate linear regression analyses adjusted for confounders, defervescence time was significantly associated with CURB-65 score (regression coefficient [B]=1.05; 95% confidence interval [95% CI], 0.09 to 2.02; p=0.033) and body mass index (B=-0.21; 95% CI, -0.40 to -0.02; p=0.030) (Table 4). Length of hospital stay was significantly associated with mechanical ventilation (B=17.07; 95% CI, 9.56 to 24.57; p<0.001) and CURB-65 score (B=4.21; 95% CI, 1.14 to 7.27; p=0.008).
In multivariate logistic regression analyses, mechanical ventilation was significantly associated with complicated pneumonia (odds ratio [OR], 37.04; 95% CI, 2.64 to 520.24; p=0.007) and CURB-65 more than 2 (OR, 8.95; 95% CI, 1.52 to 52.68; p=0.015) (Table 5). ICU care was also significantly associated with complicated pneumonia (OR, 613.85; 95% CI, 3.51 to 107,382.46; p=0.015) and CURB-65 more than 2 (OR, 46.32; 95% CI, 2.47 to 870.21; p=0.010). Mortality at 30 and 90 days were only significantly associated with FEV1% (OR, 1.05; 95% CI, 1.01 to 1.10; p=0.027; and OR, 1.03; 95% CI, 1.00 to 1.06; p=0.045) (Table 6). ICS use and blood eosinophils count were not associated with all pneumonia outcomes. Additionally, ICS type was not associated with all pneumonia outcomes in ICS users (specific data was not shown).
Discussion
We analyzed whether ICS use affected the prognosis of pneumonia in the patients with COPD. Patients were classified as ICS and non-ICS users based on their record of inhaler use prior to the development of pneumonia. ICS use did not affect the severity or outcomes of pneumonia. Clinical parameters, including initial vital signs, laboratory findings, and radiological severity, were comparable between the ICS and non-ICS users. The CURB-65 score and pneumonia outcomes, including mortality, did not differ between the two groups. These results indicated that ICS use may not be related to the poor prognosis of pneumonia in patients with COPD.
The TORCH study was conducted to examine the survival benefit of combination treatment with fluticasone propionate/salmeterol [10]. Although combination treatment improved the exacerbation of COPD, health status, and lung function; all-cause mortality, which was the primary outcome of this study, was not significantly different. Nevertheless, the TORCH study was the first study to report the increased risk of pneumonia attributed to ICS use (hazard ratio, 1.64; 95% CI, 1.33 to 2.02). Increased risk of pneumonia with ICS use was reported in many randomized controlled trials (RCTs) on COPD [11-13]. Additionally, observational studies have consistently reported an increased incidence of pneumonia in patients treated with ICS compared to those without [14,15]. The RCTs included cumulative cases of pneumonia as safety or adverse outcomes. Therefore, pneumonia was primarily diagnosed at the physicianŌĆÖs discretion, and chest radiography was not mandatory [11-13]. Observational studies using healthcare databases could not confirm pneumonia because the corresponding diagnostic code for pneumonia was used to define the pneumonia cases [14,15]. Therefore, we should cautiously interpret the study results in patients of pneumonia with COPD. An RCT previously conducted to examine the efficacy of a fluticasone furoate/ vilanterol combination was reassessed to confirm the risk of pneumonia in cases of ICS use [16]. Patients with new infiltrations on chest radiography compatible with pneumonia, which were reviewed by a radiologist, were included only as pneumonia cases. A two-fold increased risk of pneumonia was observed in ICS users compared with non-ICS users. Differentiating pneumonia from other diseases, such as COPD exacerbation and heart failure, at initial presentation with worsening dyspnea is challenging [17,18]. Real-world studies should be conducted to assess whether ICS use affects the incidence and outcomes of radiologically confirmed pneumonia in patients with COPD.
The pneumonia-related outcomes were examined in a post hoc analysis of the TORCH study [19]. Although ICS use increased the incidence of pneumonia, ICS did not affect the mortality rate, hospitalization, and length of hospitalization. Additionally, the pneumonia-related mortality rates did not vary among the other RCTs [11,12]. However, the number of cases of pneumonia and mortality rates were too small for drawing conclusions from the RCTs [20]. Retrospective cohort studies have reported conflicting results. Two studies using the National Administrative Database of Veterans Affairs reported that prior ICS use before hospitalization for CAP significantly decreased the mortality at 30 and 90 days and need for mechanical ventilation [21,22]. However, a Canadian cohort study reported that prior ICS use was associated with increased mortality and hospitalization rates attributed to CAP [23]. A prospective observational study conducted to examine the outcomes of pneumonia associated with ICS use demonstrated no difference in the pneumonia severity, systemic inflammatory markers, mortality rate, and need for mechanical ventilation between ICS and non-ICS users [24]. In contrast to previous RCTs and retrospective observational studies, only the patients admitted for CAP confirmed by new infiltrations on chest radiography along with respiratory symptoms suggestive of pneumonia were selected as pneumonia cases. The results of this study are consistent with those of our study. The initial vital signs, laboratory findings, systemic inflammation, radiologic severity, and clinical severity assessed using the CURB-65 score did not differ between ICS and non-ICS users. Additionally, the proportions of mechanical ventilation use, ICU admission, and mortality at 30 and 90 days were not significantly different. Our study results strengthen those of previous RCTs and prospective observational studies, indicating that ICS use are not associated with poor outcomes of radiologically proven pneumonia in COPD.
It is noteworthy that ICS increases the incidence of pneumonia but does not affect its prognoses. Malo de Molina et al. [22] reported decreased mortality attributed to prior ICS use before the development of pneumonia; they explained that the suppressive effect of ICS on nonspecific airway inflammation could have contributed to the better outcomes of pneumonia. Mechanistic studies have verified that ICS decreases the chemotaxis of neutrophils into the airway but maintains the functions of peripheral neutrophils, resulting in blunted airway inflammation and pneumonia severity [25,26]. However, previous prospective observational studies and our study results consistently demonstrated that the systemic inflammatory markers, including leukocytosis, C-reactive protein, procalcitonin, and clinical outcomes, did not differ. Therefore, immunosuppression with ICS could result in an increased incidence of pneumonia; however, it does not affect the outcomes of pneumonia in COPD.
Our study had several limitations. First, the small sample sizes of the study participants as ICS and non-ICS users prevents generalizing the study results and affects statistical significance. Severity and outcomes of pneumonia such as complicated pneumonia and ICU care may be significant if there were sufficient number of patients. A substantial number of patients diagnosed with COPD and pneumonia were excluded upon application of the inclusion and exclusion criteria. Approximately 40% of the screened patients did not have a record of bronchodilator use before pneumonia. As mentioned above, we confirmed the presence of cases of non-pneumonic exacerbation and incompatible with COPD based on the spirometry criteria. Therefore, our study may possess better internal validity with low bias, as we applied a narrow definition of pneumonia cases. Second, we could not determine the appropriateness of ICS use. We were unable to collect baseline healthcare records regarding the exacerbation history and laboratory findings of blood eosinophil counts before the ICS prescription. Given that ICS is overly prescribed irrespective of its indication, the outcomes of pneumonia attributed to proper use of ICS compared to those attributed to improper use of ICS may generate conflicting results.
In conclusion, ICS may not affect the severity or outcomes of radiologically confirmed pneumonia in patients with COPD. We should be vigilant when differentiating between pneumonic and non-pneumonic exacerbations of COPD. Further research is warranted to examine the pneumonia outcomes in patients stratified according to the appropriateness of ICS use.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Data Sharing Statement
Data Sharing Statement Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






