



Introduction
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 revised the definition of chronic obstructive pulmonary disease (COPD) and suggested a newly defined taxonomy, i.e., etiotypes [1]. Before GOLD 2023, the COPD definition had the following three components: (1) respiratory symptoms and airflow limitation; (2) airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases; and (3) host factors, including abnormal lung development [2]. In 2023, GOLD emphasized “heterogenous lung conditions” to embrace various causes of COPD. The main goal of this change was to uncover the heterogeneity of etiologies and pathogenesis of COPD [3]. This will allow us to provide tailored strategies to reduce exposure to various risk factors for COPD and facilitate research to reveal the heterogenous natural course of COPD according to each etiotype.
Despite the considerable disease burden, only a small percentage of individuals with COPD are diagnosed and receive appropriate care [4]. COPD disproportionately affects people in low- and middle-income countries, mostly located in Asia and Africa [5]. While tobacco smoking is the leading risk factor for COPD [6], there are many other contributing factors, such as air pollution, occupational exposure to dust and fumes, and respiratory infections [7,8]. By expanding the definition of COPD to include a broader range of heterogeneous lung conditions, it is expected that clinicians will be able to identify more individuals with COPD earlier and provide them with the appropriate preventive measures and/or treatment before irreversible damage occurs. However, there is concern about whether COPD could be used as an ambiguous umbrella term encompassing various disease entities [9]. In this review, we discuss newly proposed etiotypes of COPD and related controversy.
Change in COPD Definition and Newly Defined Taxonomy
1. History of COPD definition
Changes in major components of COPD from 2011 to 2023 are presented in Table 1. Historically, COPD has been defined as a condition characterized by persistent airflow limitation linked to noxious particles or gases [2]. However, the 2023 GOLD report updated the COPD definition to expand the boundaries of the disease in terms of etiologies [1].
Although the proportion of non-smoking-related COPD is higher than smoking-related COPD globally [5,10], COPD has been generally regarded as a smoking-related disease [8] since the development of major COPD research and clinical guidelines has mainly been driven by Western academic societies. Accordingly, COPD caused by infections and air pollution, which are more common in low-to-middle income countries, including many Asian countries, has been largely neglected by the research community. Accordingly, the previous definitions before GOLD 2023 did not fully account for these individuals. From this perspective, the revised definition of COPD seems to better define COPD by reflecting broader situations across the world.
2. Proposed taxonomy for COPD
The updated definition of COPD has led to the need for a new classification system. The GOLD committee has proposed a taxonomy for COPD that focuses on the underlying causes of the disease (Table 2). However, this definition may cause controversy since there have been no in-depth considerations for pathogenesis and clinical presentations. Some disease entities traditionally regarded as diseases distinguishable from COPD may now be included as a subtype of COPD.
Controversial Issues 1: Bronchiectasis with Airflow Limitation
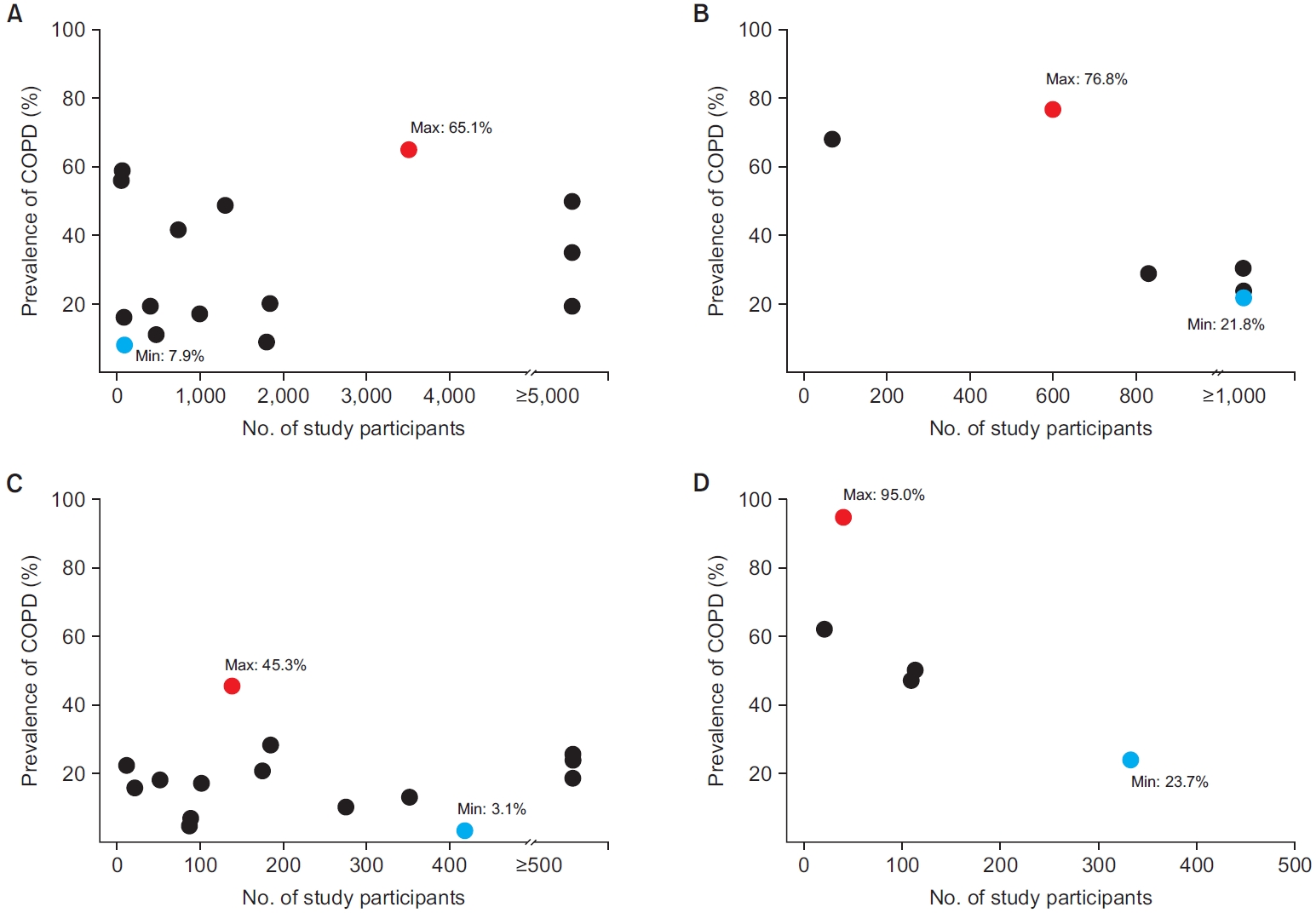
Bronchiectasis is a disease entity of clinical and radiological diagnosis (abnormal dilatation of the bronchi), characterized by cough, sputum production, and recurrent respiratory infections that overlap with other airway diseases [11-13]. The overlap between bronchiectasis and COPD is very common. A large proportion of individuals with COPD have bronchiectasis on chest computed tomography (CT) [14]. Also, a high proportion of individuals with bronchiectasis have airflow limitation or COPD (Figure 1) [15,16].
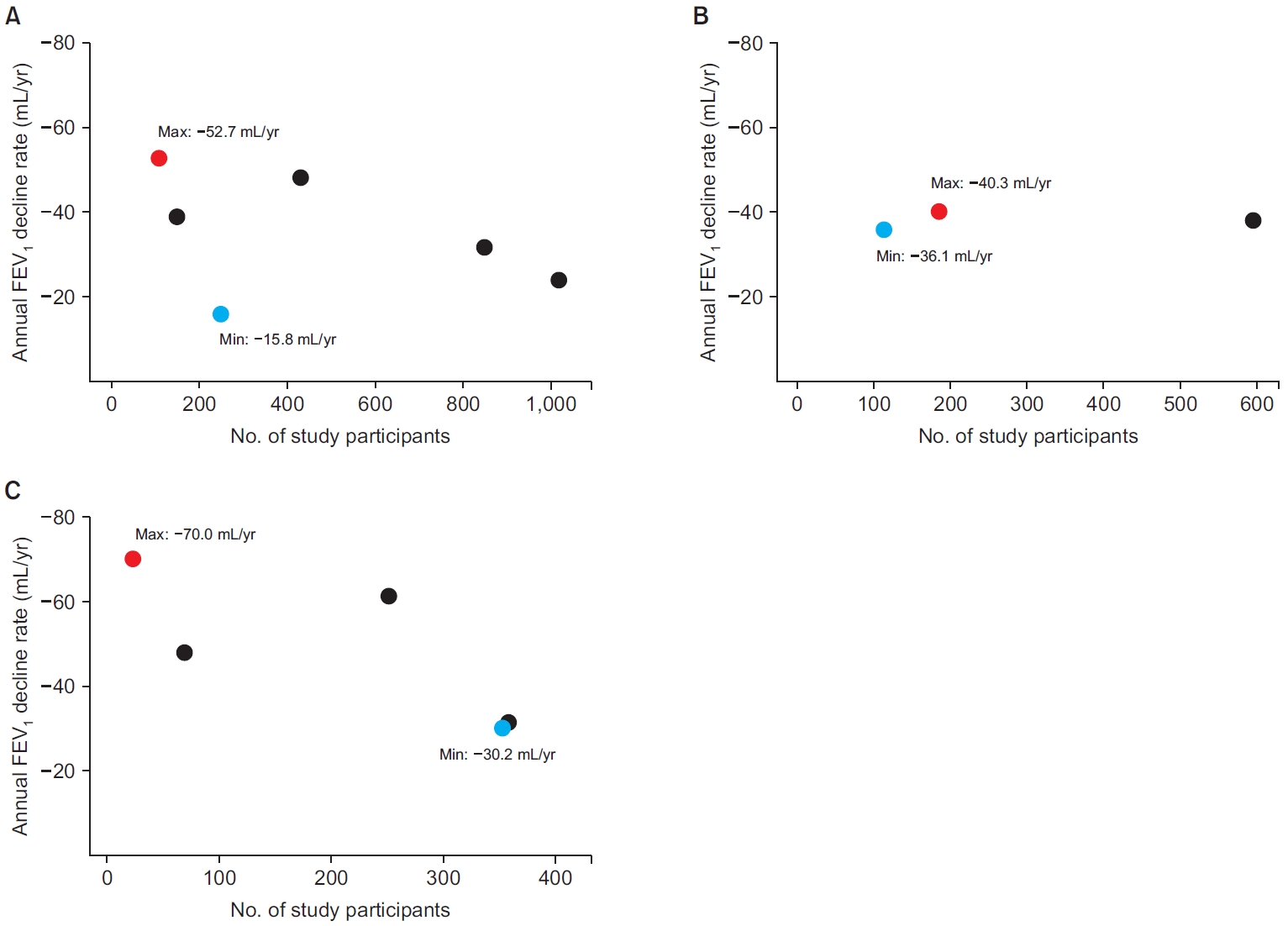
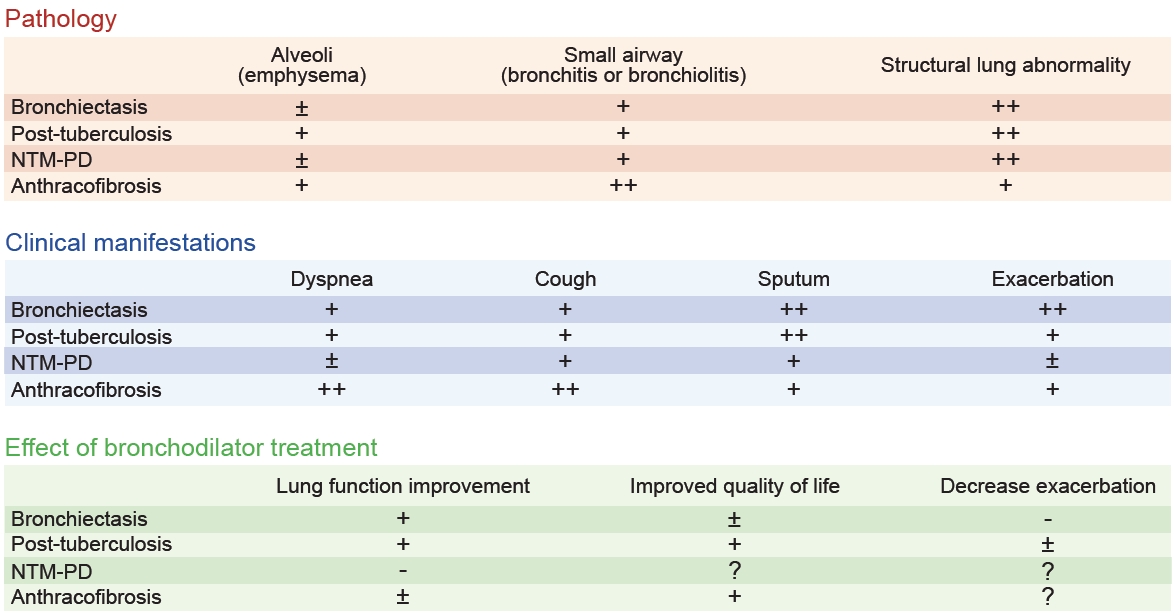
Despite a considerable overlap between the two diseases, bronchiectasis has been traditionally considered a distinct disease entity from COPD. Supporting this position, the GOLD committee mentioned that calling bronchiectasis an “etiotype” of COPD is incorrect since bronchiectasis has many causative etiologies and its own nosological entity [17], concluding that bronchiectasis represents an important comorbidity of COPD that should be identified, not an etiotype of COPD. The pathology of bronchiectasis is also different from classical COPD in terms of major involvement sites. While classical COPD is characterized by alveoli involvement and/or small airway involvement [18], the structural dilatation of bronchi is the main characteristic of bronchiectasis, although bronchiectasis is often accompanied by bronchiolitis or bronchiolitis (Table 3) [19]. Rapid lung function decline is an important pathophysiology leading to COPD. However, changes in lung function in bronchiectasis vary widely across studies (Figure 2) [20-25].
Furthermore, the main treatment strategies of bronchiectasis are also different from those of COPD, although the bronchiectasis treatment guidelines recommend using a bronchodilator in individuals with coexistence of bronchiectasis and COPD [26]. While airway clearance techniques are the cornerstone therapy of bronchiectasis treatment, the use of bronchodilators is the central management strategy for COPD [26]. Some studies have suggested that bronchodilators can be effective in improving lung function in bronchiectasis [27-29]. Although a randomized controlled trial for dual bronchodilators in bronchiectasis is ongoing [30], the effect of bronchodilators on the treatment outcomes of bronchiectasis has not been established other than lung function (e.g., quality of life and acute exacerbations) (Table 3) [31,32]. For example, although inhaled tiotropium increased lung function in individuals with bronchiectasis and airflow obstruction, it did not show reduced exacerbation or improved quality of life [27], which are all observed in classical COPD [33]. Exacerbation management is also different. In bronchiectasis, antibiotics are the main treatment, and systemic steroids are not routinely recommended [26], while in COPD, a combination of bronchodilator, systemic steroid, or antibiotics is used [8].
Despite these recommendations, a considerable proportion of experts on airway diseases suggest that bronchiectasis is an etiotype of COPD. For example, a survey of Korean experts showed that 53% of survey participants agreed with the following statement: “The definition of COPD includes patients with persistent airflow obstruction due to bronchiectasis, even without previous exposure to gases and dust, including cigarette smoking” (note: bronchiectasis mentioned here refers to patients with a main diagnosis of bronchiectasis for their respiratory condition and treatment) [34]. Although the reasons for their agreement on the statement were not provided, it seems that the experts providing agreement on the statement would have focused on the development of persistent airflow limitation and improved lung function in bronchiectasis following bronchodilator treatments [27-29].
Most studies are needed to clarify the natural course of the overlap of bronchiectasis and COPD. The coexistence of bronchiectasis and COPD leads to a higher disease burden [35], but there is currently no standardized definition for this population. Fortunately, a Delphi consensus definition for bronchiectasis-COPD overlap has recently been suggested by the European Multicentre Bronchiectasis Audit and Research Collaboration (EMBARC) Airways Working Group, which includes Radiological, Obstruction, Symptoms, and Exposure (ROSE) criteria [36]. The ROSE criteria consist of: (1) Radiological (abnormal bronchial dilatation in one or more pulmonary segments in more than one lobe and radiological findings of airway visible within 1 cm of pleura and/or lack of tapering sign); (2) Obstruction (a functional obstructive pattern [post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity <0.7]); (3) Symptoms (two or more of the following symptoms [cough, expectoration, dyspnea, fatigue, and frequent lower airway infections]); (4) Exposure (ever smoker with more than 10 pack-years or other toxic exposure). Future studies using this definition would provide more evidence of the relationship between the two diseases while reducing the heterogeneity of clinical characteristics of the study population caused by different definitions of bronchiectasis-COPD overlap.
Controversial Issues 2: COPD Due to Infection
In the revised GOLD 2023 guideline, childhood infection, tuberculosis (TB), and human immunodeficiency virus (HIV)-associated airflow limitation are proposed as examples of COPD due to infection (COPD-I). Traditionally, obstructive lung disease caused by those diseases was not classified as COPD, even though infection-related obstructive lung diseases are frequently encountered in real-world clinics. With accumulating data on the association between these three infectious conditions and COPD, classifying this disease entity into COPD-I is reasonable, and it is welcome news that we now have a rationale on which to base various preventive modalities and treatments for individuals with COPD-I. For tuberculosis-associated COPD, we focus on the accumulated evidence on the relationship between COPD and TB rather than a controversial issue. We will discuss controversial issues on COPD related to other respiratory infectious conditions (e.g., non-tuberculous mycobacterial pulmonary disease [NTM-PD]).
1. Tuberculosis-associated COPD
Pulmonary TB is an important cause of airflow limitation in Korea; Rhee et al. [37] found that approximately 75% of individuals with a TB-destroyed lung (TBDL) had airflow limitation. Another Korean study also showed that evidence of previous TB on chest X-ray was associated with increased odds of airflow limitation even after adjustment or exclusion of smokers [38]. Regarding the overall risk of COPD in post-TB individuals, a meta-analysis of studies evaluating the association between pulmonary TB and the risk of COPD found that individuals with a history of pulmonary TB had a 2.59-fold increased risk of developing COPD [39]. In studies using the Korean National Health Examination Survey data, a history of pulmonary TB was frequently observed in individuals with airflow limitation [40,41]. Likewise, COPD is prevalent in the post-TB cohort [38,42,43]. While the size and enrollment criteria for subjects who have experienced pulmonary TB vary across studies, the prevalence of COPD in individuals with a history of pulmonary TB ranges from 21.8% to 76.8%, indicating a close connection between both conditions (Figure 1) [37,44-48]. Also, a relatively consistent and fast decline in lung function of about -40 mL/year in FEV1 has been reported post-TB individuals [37,49,50], which is higher than the FEV1 decline in Korean healthy never smokers (-31.8 mL/year) [51].
Previous COPD definitions, including a history of exposure to noxious particles as a criterion, led to a debate about whether airflow limitation observed in post-TB individuals can be regarded as COPD. However, growing evidence shows that post-TB with airflow limitation could be classified as COPD-I. Park et al. [52] investigated the impact of a history of pulmonary TB on the severity and outcomes of COPD using the Korean COPD cohort. The prior TB group had worse respiratory symptoms and quality of life, lower lung function, and increased prevalence of exacerbation compared to the non-TB group. Pathology also supports that post-TB airflow limitation should be classified as COPD-I because they have alveoli involvement as well as small airway pathologies (Table 3) [53]. Additionally, bronchodilators, a cornerstone therapy for COPD, significantly prevented future lung function decline and improved COPD outcomes in individuals with COPD accompanied by TBDL [54]. Although the prevention effect of bronchodilators for exacerbation was unclear, using bronchodilators was also associated with a decrease in mortality among this population (Table 3) [55,56]. These findings align with the new concept that post-TB-related airflow limitation may be a distinct subtype of COPD.
2. Other respiratory infections: NTM-PD
Certain chronic respiratory infections other than pulmonary TB may be linked with COPD, indicating the potential existence of COPD-I other than COPD related to childhood infection, HIV infection, and TB. Although other infection-related airflow limitation were not included in the guideline, the GOLD committee commented that various infections could be causes for COPD development, and NTM-PD is one such candidate [17]. NTM-PD is a chronic infectious lung disease characterized by its persistence and slow-progressing nature, with its prevalence and disease burdens steadily rising [57]. The airflow limitation is frequently encountered in the management of NTM-PD. In a study of 358 individuals with NTM-PD, 8.2% of subjects experienced a change in lung function from normal to obstructive during a median 5.6-year follow-up [58]. In the NTM studies evaluating COPD as a comorbidity, the comorbid COPD was reported up to 65.7% in individuals with NTM-PD [59-73], suggesting a comparable prevalence of COPD within individuals with TBDL (Figure 1). In contrast, NTM-PD was also found in individuals with COPD, and comorbid NTM-PD is associated with poor prognosis [74,75]. Moreover, the decline in lung function is often pronounced in individuals with NTM-PD (Figure 2) [58,75-78]. As in TB, NTM-PD shares common features of pathologic changes in COPD, such as alveoli involvement and small airway involvement [79]. However, information on the treatment response to bronchodilators is scarce in individuals with NTM-PD (Table 3).
There is very little literature that highlights the underlying mechanism linking COPD and NTM-PD. There may be a bidirectional association between these two diseases, promoting the development of each condition by the other condition. NTM-associated airway inflammation may cause small airway obstructions [80], and in individuals with COPD, defense against the pathogen is reduced [81]. Nevertheless, there are distinguishing features in NTM-PD associated with airflow limitation from classical COPD. First, antimicrobial agents remain the main treatment for NTM-PD [82]. The role of bronchodilators has not been established in NTM-PD, even when the individuals have airflow limitation [58]. Additionally, airflow limitation might be improved through appropriate infection control [83]. Second, considering these chronic respiratory infections commonly exist as a comorbid condition of structural lung disease, most airflow limitation in these populations may be associated with underlying lung parenchymal destruction [28]. Third, the natural course and clinical outcomes are mainly driven by the features of NTM (NTM species, cavity, acid-fast bacilli smear positivity, etc.) rather than those of COPD [84].
In this context, COPD may be an under-recognized condition in the management of NTM-PD, but it is uncertain whether NTM-PD could be classified as COPD-I. More studies will be required to classify NTM-PD-associated airflow limitation as COPD-I.
Controversial Issues 3: COPD Due to Environmental Exposure
1. Bronchial anthracofibrosis
Bronchial anthracofibrosis (BAF) is a chronic lung disease caused by the inhalation of fine particles of carbon from biomass fuel smoke [85]. BAF is commonly found in elderly women who are never smokers and live in low- and middle-income countries where biomass fuels are commonly used for cooking and heating [86]. Also, several studies reported the association between pulmonary TB and BAF [85]. This disease entity is often diagnosed as asthma or COPD because of similar spirometric findings, i.e., obstructive spirometry pattern [87].
The prevalence of airflow limitation in BAF varies widely; most studies reporting spirometric results in BAF were conducted based on a relatively small number of individuals, and the prevalence of airflow limitation was 24% to 95% (Figure 1) [88-90]. In Korea, the rate of having BAF in COPD seems relatively frequent. According to a single-center respective study in Korea, one-fourth of the individuals had a BAF based on CT criteria among the those with COPD exacerbation [87]. From a pathologic view, BAF and COPD both commonly affect small airways despite their distinct patterns of pathological changes (Table 3) [91].
However, some features of BAF are different from those of classical COPD. First, although not frequent, BAF occasionally involves larger airways and regional mediastinal lymph nodes, which leads to mechanically obstructive lung disease rather than a small airway disease. In those cases, bronchoscopic intervention (e.g., mechanical dilatation of a large airway) has a central role in the treatment of BAF [92]. Second, the effects of bronchodilators are less significant than those in individuals with COPD. While some research demonstrated the effect of bronchodilators, unresponsiveness to bronchodilators is more commonly reported (Table 3) [93,94]. Therefore, more studies are needed on whether this condition can be classified as COPD-P.
2. Pneumoconiosis
COPD frequently coexists with pneumoconiosis, raising the question of the prevalence of COPD in individuals who suffer from pneumoconiosis. Several studies reported a common occurrence of airflow limitation, suggesting COPD in individuals with pneumoconiosis, with the prevalence of COPD being around 20% [95]. In light of the latest taxonomy for COPD, such cases might be classified as COPD-P. However, some issues should be considered before classifying pneumoconiosis as a COPD-P. First, pneumoconiosis has a distinctive clinical manifestation, with progressive massive fibrosis being the most prominent example [95]. Progressive massive fibrosis is a severe form of pneumoconiosis where large amounts of the lung tissue turn fibrous, impairing its function [96], which is different from classical COPD. Second, the underlying pathology of lung dysfunction in pneumoconiosis may differ from that of classical COPD. Pneumoconiosis is often a result of prolonged exposure to relatively large dust particles, leading to specific structural changes in the lungs, which is distinguished from the small airway dysfunction in COPD [97]. Lastly, pneumoconiosis is not a single disease entity. There is heterogeneity among diseases in the pneumoconiosis category [97]. Besides, the impact of bronchodilator treatment on the treatment outcomes in individuals with pneumoconiosis-related airflow limitations has not been studied.
Conclusion
The 2023 GOLD Committee revised the definition of COPD to reflect its heterogeneity of etiologies and pathogenesis and to enable tailored strategies reducing exposure to COPD risk factors across various etiotypes. Accumulating evidence agrees with the suggestion by the GOLD committee that TB is an important etiology of COPD-I. However, there may be controversy in classifying some diseases, such as bronchiectasis, respiratory infections other than TB, BAF, and pneumoconiosis, as etiotypes of COPD. Future research is warranted to clarify the role of these diseases in COPD development and progression.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Print
Print Download Citation
Download Citation






